


It’s 3 a.m., and you’re scrubbed in for an emergency operation. The patient is septic, hemodynamically unstable, and requires a complex, lifesaving bowel resection due to a strangulated ventral hernia after an abdominal wall reconstruction case. The recurrence—which occurred after their initial repair—has become a catastrophic, life-threatening event.
Now, imagine the patient you saw yesterday in clinic: a healthy, 60-year-old on a routine follow-up after an abdominal wall reconstruction following a liver transplant. An abdominal CT, performed for unrelated reasons, incidentally revealed a small 1-cm fascial defect near the original repair site. The patient is completely asymptomatic, has no pain, and is unlikely to ever require surgical intervention.
In the eyes of the current surgical literature, both scenarios—the near-fatal strangulation and the benign, asymptomatic finding—are counted the same way: as a hernia recurrence.
For too long, the scientific literature has clung to a simplistic, binary “yes or no” reporting system. This reductive approach is worse than just unhelpful; it’s a fundamental failure to capture the true clinical complexity, patient morbidity, and severity of the hernia disease. The avoidance of a hernia recurrence is, rightly, the most desirable outcome after abdominal wall reconstruction, prompting all hernia publications to quote recurrence rates. However, by reporting recurrence as a dichotomous outcome, we are essentially ignoring the clinical history and neglecting the patient’s quality of life (QOL) when recurrence occurs. There is an urgent need for more granular information on the QOL of patients with hernia recurrence and a parallel requirement for standardization to allow for honest comparisons of future studies.
This lack of precision not only confuses researchers; it affects clinical decisions, makes benchmarking surgical quality impossible, and ultimately fails our patients. When recurrence rates after ventral hernia repair are estimated as high as 40% with mesh repair and 70% without mesh repair at five years postoperatively, we must demand better reporting tools.
That is why we developed and published the hernia recurrence classification system (Hernia 2025;29[1]:265). This is more than a new academic framework; it is a necessary tool for every general surgeon who wants to standardize care, better manage their patients, and finally treat hernia as a complex chronic disease. Our objective is clear: to propose a novel classification for hernia recurrence after ventral hernia repair that reflects the clinical reality.
The Inadequacy of Dichotomy: Why We Need a Common Language
In surgery, we rely on standardized classification systems for good reason. They are used as an objective measure to evaluate improvement in standard surgical procedures and allow for comparison of results among centers. Why? Because recurrence is one of the main postoperative complications after a hernia repair and is a surrogate for surgical quality.
Consider the monumental impact of the Clavien-Dindo classification for postoperative complications. Its widespread adoption led to more than 200 studies using the system within five years of its second publication, significantly improving the communication and standardization of reporting surgical outcomes. This is the power of a common language: It allows for consistent comparison of outcomes across studies, enhancing transparency and collaboration.
Hernia recurrence must follow suit. The two main benefits of the new system are simple: to create a standardized language to improve communication, and to provide improved guidance to surgeons regarding the need for or against surgical intervention.
Improving QOL: A Patient-Centric Approach
The hernia recurrence classification was born from the recognition that recurrence often leads to “decreased QOL” and years of “chronic pain,” underscoring that a recurrence is not just a defect but a major clinical event driven by the clinical history of patients. Unlike previous reporting methods, the system’s primary focus is on the clinical relevance of the recurrence and resulting need for intervention, making it broadly applicable across all types of ventral hernia repair. The sequential, six-grade structure provides improved guidance to surgeons on intervention, ranging from Grade I (asymptomatic), which covers incidental findings (IA) or patient-reported but asymptomatic defects (IB). The severity progresses to Grade II (symptomatic—elective), where symptoms guide the decision for watchful waiting (IIA) versus an elective repair (IIB). The system escalates to Grade III (urgent) for same-admission repair and culminates at Grade IV (life-threatening/emergent), which mandates immediate, lifesaving surgery for catastrophic complications like strangulation or septic shock (Table). This granular scale allows surgeons to move beyond the binary failure model and accurately tailor patient counseling and surgical planning based on the true burden of the recurrence.
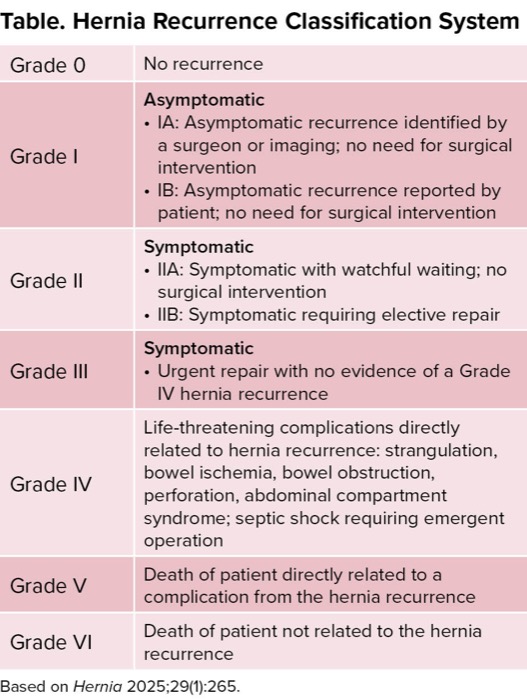
| Table. Hernia Recurrence Classification System | |
| Grade 0 | No recurrence |
| Grade I | Asymptomatic
|
| Grade II | Symptomatic
|
| Grade III | Symptomatic
|
| Grade IV | Life-threatening complications directly related to hernia recurrence: strangulation, bowel ischemia, bowel obstruction, perforation, abdominal compartment syndrome; septic shock requiring emergent operation |
| Grade V | Death of patient directly related to a complication from the hernia recurrence |
| Grade VI | Death of patient not related to the hernia recurrence |
| Based on Hernia 2025;29(1):265. | |
The Research Revolution: Chronic Disease and Clear Benchmarks
As long-term data, well beyond five years, are being reported, many of us are now accepting the fact that hernia isn’t just a single acute injury; it’s a chronic and long-term process that the scientific community still needs to better understand. That means our research must evolve as well. Right now, long-term follow-up is brutal; it’s difficult to obtain, and something called attrition bias (in which patients drop out of studies) plays a big role, especially in cohort studies on abdominal wall reconstruction.
This classification system ensures that. More than that, it finally gives us the scientific clarity we need for benchmarking. We can stop arguing over a vague 5% recurrence rate! We can now compare a recurrence rate of 5% in Grade IIB (elective surgery needed) versus 5% in Grade IV (life-threatening emergency) and definitively determine which repair technique is truly safer and better for the patient. This helps us generate data that show not just which technique fails less often, but which one fails less dangerously and imposes a lower clinical burden. While collecting all these data and fighting attrition bias are challenging, this uniform grading system may help scientific communication by giving us a clear, shared framework, even when dealing with imperfect follow-up.
A Call to Action: Start Grading Hernia Recurrences Today
The conclusion is straightforward: Recurrence should no longer be assessed as a simple “yes/no” variable. It must be assessed in a more granular way. We must distinguish it “as an incident finding with no clinical repercussions for the patient,” or “as a true complication with deterioration QOL for patients.”
This is a novel theory; it’s the first study to propose such a classification. Like any great advance, it still needs to be validated over time with multicenter data. We need to see it used widely across institutions and surgical registries and accepted by hernia societies worldwide.
We have formulated this classification and its subgroups to better understand the clinical outcomes of patients with recurrence after ventral hernia repair and to unify criteria among surgeons when describing it. This is a commitment to precision, patient safety, and scientific honesty. Let’s adopt this language now, start collecting the detailed data, and finally give our hernia patients the comprehensive, long-term care they deserve.
Dr. Docimo is an associate professor of surgery; the vice chair of surgery, quality; the section chief of abdominal wall surgery; and the associate director of the Bariatric & Foregut Fellowship at the University of South Florida, in Tampa.
Dr. Docimo reported receiving honoraria from BD, Boston Scientific, Intuitive, and Medtronic.
This article is from the December 2025 print issue.
Please log in to post a comment