

ORANGE, Calif.—A working group from the American Foregut Society reviewed and expanded the Hill grade classification to aid in the characterization and treatment of patients with gastroesophageal reflux disease. A white paper describing the new classification was published in Foregut (2022 Sep 28. doi:10.1177/26345161221126961).
“GERD is one of the most common chronic esophageal disorders, and endoscopy is one of the best ways to document the anatomic changes of the esophagogastric junction [EGJ] that are correlated with the presence of GERD. Therefore, it is important to have a user-friendly classification system that can document the anatomic findings of the EGJ during routine upper endoscopy,” said lead study author Ninh Nguyen, MD, the chair of the Department of Surgery at the University of California, Irvine.
The Hill grade is an endoscopic classification that was developed to grade the gastroesophageal flap valve, but its use has been suboptimal, explained Christy Dunst, MD, an esophageal surgical specialist at The Oregon Clinic in Portland.
“The original classification by Dr. Hill provides the framework for discussing the anatomic integrity of the gastroesophageal flap valve, but, unfortunately, its routine use has not been widely adopted by the endoscopy community. Surgeons are typically more well versed in the Hill classification but find it lacking in some key structural components such as hiatal diameter, degree of EGJ migration (hernia), etc. that impact antireflux surgery,” Dr. Dunst said.

A team of 13 experts in foregut disease from gastroenterology and gastrointestinal surgery convened to review and update the Hill classification. After their review, the working group came to an agreement on the pathophysiology of the antireflux barrier.
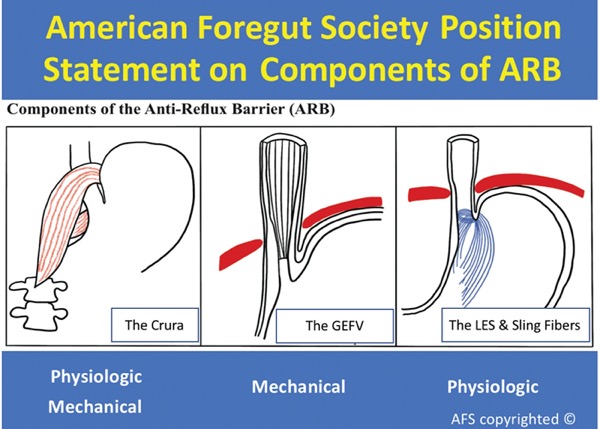
“This group of experts agree that GERD is related to an impairment of the antireflux barrier, which is comprised of the flap valve, the crura of the diaphragm, and the lower esophageal sphincter and its gastric sling fibers,” Dr. Nguyen said. “Together, these three components contribute to the mechanical and physiologic barrier to reflux.”
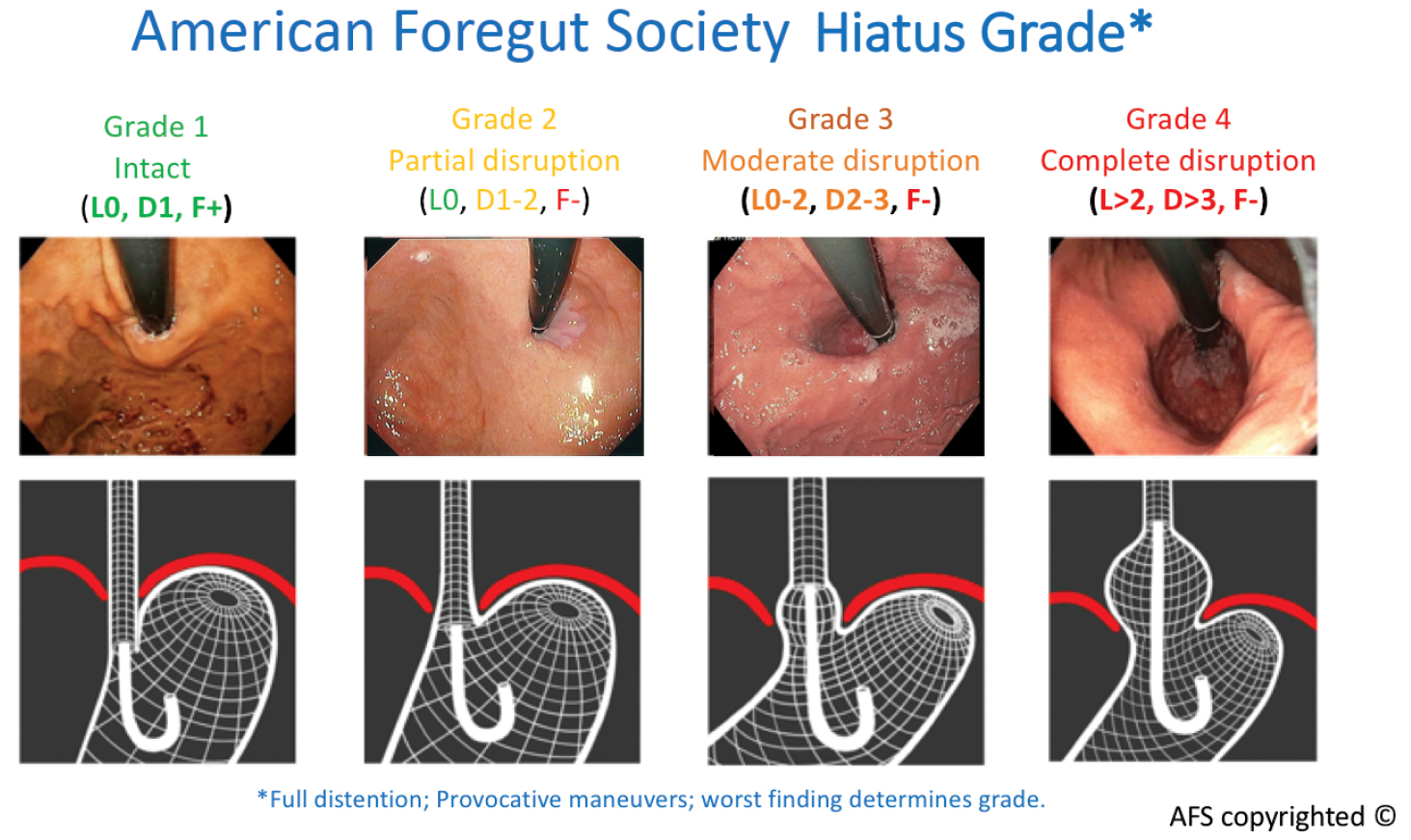
The new classification considers this pathophysiology and stratifies EGJ integrity across four grades. Grade 1 is normal, while grades 2 to 4 describe increasing degrees of EGJ disruption.
Although the Hill classification is based on visual characterization of the gastroesophageal flap valve seen via the retroflexed endoscopy view, this new classification improves upon the Hill classification by not only considering the presence or absence of a flap valve, “but also documenting the presence and degree of hiatal disruption,” Dr. Nguyen explained.
In addition to requiring examination for the presence or absence of a flap valve and measurement on the degree of hiatal disruption to obtain an accurate assessment of the hiatus, the classification system requires full endoscopic insufflation and rotational provocative maneuvers in the retroflex view to elicit potential hiatal herniation.
“Since this new classification takes into account both the presence or absence of a flap valve and the degree of hiatus disruption, the final hiatus grade is based on the worse findings,” Dr. Nguyen said. “A patient with a 1.5-cm axial length hiatal hernia will automatically jump to a hiatus grade 3. In the Hill grade classification, you can observe a Hill grade 1 flap valve while also having a 1-cm hiatal hernia axial length. In this new classification, this scenario is not possible.”
“A comprehensive evaluation of the components of the reflux barrier is very important to planning structural repair. This was less important decades ago when we had a ‘one-surgery-fits-all’ approach with Nissen fundoplication. But now with advancements in techniques, the choice of repair can be tailored to the individual anatomy,” Dr. Dunst noted.
Dr. Nguyen hopes that this new classification will encourage more endoscopists to routinely document anatomic changes in the EGJ on the endoscopy report.
“Currently, less than 20% of endoscopy reports have documentation of the anatomic view of the hiatus,” he said.
Dr. Nguyen said next steps include performing validation studies to understand the correlation between hiatus grade and the presence and degree of GERD, and grading the hiatal appearance in patients who have undergone prior antireflux intervention.
“My career has been dedicated to this topic for nearly 20 years. I love seeing the enthusiasm for this complex 2 inches of the human body,” Dr. Dunst said. “With more eyes investigating the intricacies of the interplay between the flap valve, the lower esophageal sphincter and the diaphragm, the field will advance with less invasive, more effective early treatments for millions of people suffering with GERD. It’s an exciting time.”
This article is from the January 2023 print issue.
Please log in to post a comment