

AUSTIN, Texas—Figuring out which type of ventral hernia repair the patient standing in front of you with a recurrence originally had may require many forms of information, including radiographic images, operative notes and patient engagement. Surgeons tested on imaging alone are accurate less than half of the time, according to research discussed at the 2023 annual meeting of the American Hernia Society (Hernia 2023;27[2]:347-351).
When Kaela Blake, MD, was a fellow at Cleveland Clinic, she and a team of researchers led by Michael Rosen, MD, set out to evaluate whether surgeons can accurately identify the type of ventral hernia repair a patient had previously undergone based solely on the patient’s imaging findings.
“We asked 15 expert abdominal wall repair [AWR] surgeons across the country at 10 different institutions to review 21 axial CT scans of patients who had undergone ventral hernia repair and gave them a multiple-choice test asking which hernia repair the patient previously had,” said Dr. Blake, now a hernia surgeon and an assistant professor of surgery at the University of Tennessee Medical Center, in Knoxville.
The repairs were robotic intraperitoneal onlay mesh (IPOM), robotic total extraperitoneal, or eTEP, open Rives-Stoppa, open anterior component separation and open transversus abdominis release (TAR). Other options included a positive control with a prior laparotomy without a hernia repair, and a negative control with no prior abdominal surgery. Each of these options was represented three times, for the total of 21 scans.
The main outcome assessed was surgeon accuracy, followed by interrater reliability (agreement among surgeons), and repeatability—whether an individual surgeon could identify the same type of repair in a reproducible manner.
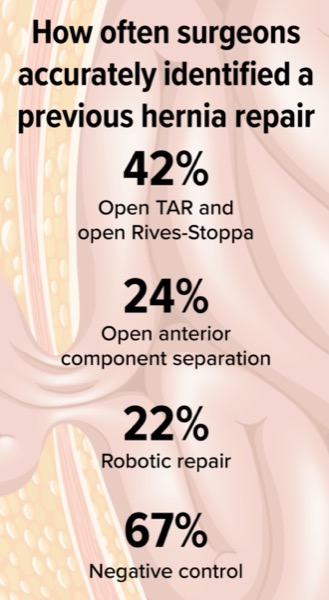
The surgeons were accurate in identifying open TAR and open Rives-Stoppa repairs 42% of the time, open anterior component separation 24% of the time, and robotic repair 22% of the time, and were correct at identifying 67% of the negative controls.
“So, less than 50% of the time could expert AWR surgeons identify the correct type of ventral hernia repair done previously,” Dr. Blake said. “Surgeon agreement was fair, but they were often incorrect when they did agree.” Repeatability was poor.
From these findings, Dr. Blake suggested that it’s quite challenging for surgeons to accurately determine the type of hernia repair the patient had when operative notes are incomplete or missing.
“It’s really hard. A lot of the time it’s not until we get into the operating room that we figure out what actually happened. When we dictate our operative notes, it’s important for us to include what type of mesh we used, where we placed it and how big it is to help each other out—and use the resources you have to use to get those operative notes.”
Eric Pauli, MD, the David L. Nahrwold Professor of Surgery and chief of the Division of Minimally Invasive and Bariatric Surgery at Penn State Health Milton S. Hershey Medical Center, in Hershey, Pa., said the study findings could be interpreted in many ways. “The first question you want to ask is, ‘Is 50% good or bad?’ The only other person interpreting those studies is the radiologist, and we know radiologists miss hernias, misinterpret hernias and misreport hernias. That’s partly why we encourage hernia surgeons to look at their own films.”
Dr. Pauli, who was one of the subjects in the study, also noted that the circumstances under which subjects evaluated the images were not those that surgeons experience in real life. “It was a bit of a false situation. Rarely, if ever, do I look at an imaging study alone without having communicated with and examined the patient and getting their operative reports. It would be extremely unusual for an expert hernia surgeon to ever just look at the films and render an opinion about what’s going on.”
He noted that the study further emphasizes points he and others tell their colleagues in general: Get the operative notes, read what surgeries the patient had, and talk to and examine the patient. “When you put those things together—the patient and the physical exam, the imaging and the operative notes—only then can you make an assessment about what’s going on to do a successful hernia recurrence repair.”
Dr. Pauli acknowledged, however, that getting and reviewing the operative notes doesn’t always provide the level of enlightenment a surgeon would hope for. “Operative notes in general are very poor. They reflect the surgery, but not always the details that matter most.”
In hernia surgery, these details include the size of the hernia, type of procedure done and whether mesh was used; if so, where and how the mesh was placed and its size. “When you review operative reports, the most commonly used mesh is called ‘appropriately sized mesh.’ That is both a joke but also the truth,” Dr. Pauli said.
These reasons are why he relies on all three aspects—the patient, notes and imaging—to figure out why the earlier surgery failed and what he needs to do differently to fix it. “Part of what I enjoy in hernia surgery is that there is a bit of detective work in figuring this stuff out.”
This article is from the April 2024 print issue.
Please log in to post a comment