

SAN FRANCISCO—Common bile duct injury (BDI) can be devastating for patients, involving complications, reinterventions, hospitalizations and mortality risk. It also imposes a significant financial burden and is the leading reason that general surgeons get sued for malpractice, especially when the injury is missed, said Michael Brunt, MD, the Pruett Professor of Surgery at the Washington University School of Medicine in St. Louis.
Brendan Visser, MD, a professor and the section chief of hepato-pancreato-biliary surgery at Stanford University School of Medicine, in California, stated it this way: “Bile duct injuries continue to be a real area of concern for general surgeons—a ‘there but for the grace of God, go I’ complication.”
At the 2024 annual meeting of the American College of Surgeons, experts in the management of BDI discussed strategies for avoiding the injury and for dealing with BDI during the initial surgery, soon after or following a substantial delay.
Minimizing the Risk for BDI
“Having experienced a major BDI in the early 1990s, before [Dr.] Steve Strasberg described the critical view of safety, I’ve been passionate about this topic my whole career,” Dr. Brunt said.
The drive to prevent BDI led Dr. Brunt and his colleagues to establish the Society of American Gastrointestinal and Endoscopic Surgeons’ safe cholecystectomy program to minimize the risk for BDI and other injuries. To this end, he and other experts held a multi-society, state-of-the-art conference that resulted in the development and publication of evidence-based guidelines for the prevention of BDI (Ann Surg 2020;272[1]:3-23 and Surg Endosc 2020;34[7]:2827-2855).
The group also developed a six-step program with the same goal in mind. “The greatest thing you can do to minimize BDI is to follow these six steps,” Dr. Brunt said.
Step 1. Understand and apply the critical view of safety.
“BDI is a misperception injury. The surgeon thinks he or she is looking at the cystic duct when it’s actually the common bile duct,” Dr. Brunt said. “Often a portion of the duct gets excised before it’s recognized, and the right hepatic artery can be injured as well.”
Step 2. Understand aberrant anatomy.
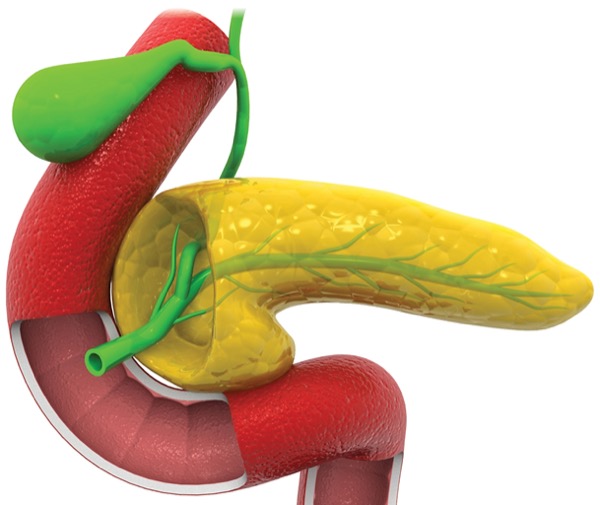
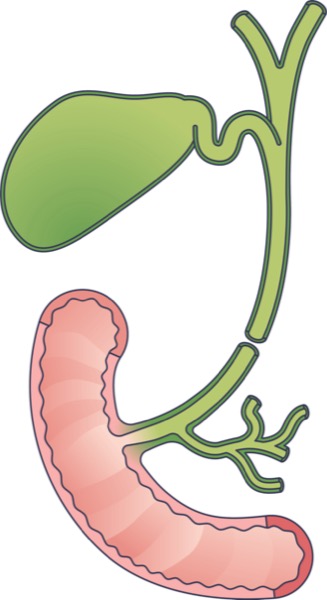
Some aberrant anatomy includes low insertion of a right bile duct; a large peripheral duct that runs just underneath the liver bed; and Rouviere’s sulcus, “an anatomic landmark we may not think about enough, which represents the fissure on the liver between the right lobe and the caudate,” Dr. Brunt said. “It marks where the right portal pedicle enters the liver, and it also indicates the plane of the bile duct. Dissection should always occur anterior, or ventral to the plane of that sulcus.”
Step 3. Take a momentary pause.
“Before you reach a step from which you can’t go back—i.e., clipping and cutting the ductal structure—ask yourself, ‘Is what I’m looking at what I really think I’m seeing?’”
Step 4. Liberal use of cholangiography or other imaging of the biliary tree.
“There’s good data that shows it might reduce the risk of injury [BMJ 2012;345:e6457]. Particularly in the setting of uncertain anatomy or suspicion of a BDI, it may prevent you from making a small injury into a bigger one and excising a portion of the biliary tree.”
Step 5. Recognize when you may be in danger and need to shift your approach.
“We know the conditions associated with a difficult gallbladder: morbid obesity, acute cholecystitis, severe chronic cholecystitis and contracted gallbladder, Mirizzi’s syndrome, and cirrhosis,” Dr. Brunt said. A consensus recommendation for managing these patients at high risk for surgery in the acute setting is to delay surgery. “Put in a percutaneous cholecystostomy tube, let things settle down and come back another day.”
Dr. Brunt noted that converting to open doesn’t necessarily guard against BDI, and that subtotal cholecystectomy is warranted in some cases. “You never have to take out the whole gallbladder for a benign disease when the potential risk exceeds the benefit.”
Step 6. If you suspect you have a BDI during laparoscopic cholecystectomy, get help.
“If you’re not experienced with biliary reconstruction, you should probably stop and just put a drain in. The patient should be transferred to a center with a hepato-pancreato-biliary surgeon and an interdisciplinary team with interventional endoscopy and radiology. That’s a strong recommendation.”
Intraoperative Management of BDI
Intraoperative recognition and management of BDI are paramount for good outcomes, but outside the hands of an HPB surgeon with an interdisciplinary team, the best strategy remains controversial and challenging, said Pablo Valsangiacomo, MD, an associate professor of surgical clinic with the Maciel Hospital School of Medicine, in Montevideo, Uruguay.
“What we want to answer is, what does a general surgeon need to know? What should you do or not do? And how do you stay calm and do no harm?” he noted.
Although most BDIs are discovered postoperatively, repair at the time of surgery is associated with better long-term effectiveness, less morbidity, lower mortality, decreased expense and improved patient quality of life, so it’s crucial to recognize when something isn’t right, Dr. Valsangiacomo said. He gave examples: “when the clip is insufficient to occlude the ductal structure, or the ductal structure being dissected can be traced without interruption behind the duodenum, or the operative field reveals another duct, or when more than eight clips have been placed.”
When a BDI has occurred, the diagnosis can made be directly, for example, when bile leaks from the hepatic duct, or indirectly, when cholangiography shows a leak or loss of continuity of ducts in any sector of the hepatic biliary tree, he said.
The strategy for intraoperative repair is based on several factors: the time of diagnosis of injury, the type and mechanism of injury, the patient’s condition, and the surgeon’s expertise. “When injury has occurred, it’s important to perform intraoperative cholangiography. If the duct is less than 3 mm, we recommend simple ligation; if the duct is more than 4 mm, we recommend a surgical repair,” Dr. Valsangiacomo said.
Similarly as Dr. Brunt stressed, if an HPB surgeon is not available, “place a drain and transfer the patient to a referral center,” he said.
Early Postoperative Management of BDI
Bile duct injuries discovered within six weeks after surgery fall into two categories: 1) minor injuries, in which there was partial dissection of the biliary tract, no loss of tissue, and that may not require surgical intervention, and 2) major injuries, associated with total dissection of the bile duct and loss of tissue, according to Pablo Cantileno, MD, an assistant professor of surgery at Maciel Hospital, Universidad de la Republica Oriental del Uruguay, in Montevideo.
“With minor BDI, if the surgeon leaves a super hepatic drain, we can administer antibiotics and monitor the patient. Patients without a drain usually require an abdominal drain for the biloma that develops,” he said, noting that if symptoms worsen, the patient may be treated endoscopically by sphincterotomy or stent placement.
With a major BDI, several factors come into play: the general and local conditions of the patient, time of diagnosis, whether the BDI is associated with a vascular injury, and whether there is access to an HPB surgeon.
“The optimal timing of a definitive repair remains under debate. Most surgeons recommend a repair within 72 hours because we have better patient [quality of life], low rates of readmission and less cost,” Dr. Cantileno said. Intermediate repairs, between weeks 1 and 6, are not recommended.
“When we make the diagnosis after 72 hours, the recommendation is to delay repair until after six weeks out to six months. There is some retrospective research that found no difference in the timing of biliary repair, while others recommend a late repair for a better long-term prognosis,” he said.
The gold-standard repair for BDI diagnosed postoperatively is a hepatic jejunostomy Roux-en-Y. “Other techniques have worse results and greater incidence of a stricture. The repair can be made via laparotomy, laparoscopy or robot depending on the experience of the surgeon and the resources of the hospital,” Dr. Cantileno said.
“As general surgeons, we need to be familiar with this topic, to know what to do and what not to do. If you lack experience, don’t panic—place a drain and refer the patient as soon as possible to a tertiary center. We need stronger evidence to support the timing of definitive repair, and we need to focus on prevention,” he noted.
Reasons to Delay Repair
There is little doubt that under the right circumstances—a stable and optimized patient without acute inflammation or vascular injury—early repair is preferable, for both patients and surgeons, Dr. Visser said.
“It changes the whole course of that patient’s disease and recovery. Those repairs, when done in experienced hands, have a 90%-plus long-term patency, which truthfully avoids some of the medical–legal downstream consequences for that operating surgeon.”
But there are some circumstances when early repair isn’t optimal or possible. One is delayed recognition by the initial operating surgeon, or by whomever is managing the patient in an era of increased rotation of surgical staff and of hospitalist management, Dr. Visser said.
“It’s really critical that we maintain responsibility for patients we have operated on, and that operating surgeons identify those injuries as soon as possible.”
Another form of delay is transferring patients to tertiary hospitals. “We often don’t have a bed. Patients can wait 48 to 72 hours just to get the bed,” Dr. Visser said.
There’s also the problem of a patient not being fit for another surgery—one who is still unwell from their cholecystitis, or from the BDI and its sequelae, and those who have vascular injuries. “Complex injuries may need some time to really explore and understand with radiology studies before you dive into the OR,” Dr. Visser said.
Turning to the medical literature for guidance on early versus late repair might produce more questions than answers. Much of the research dates to the initial era of laparoscopic cholecystectomy BDI; it tends to be retrospective in nature; and some data sets include patients managed endoscopically or by other means. “It’s a little difficult to tease apart patients who required hepaticojejunostomy from the ones that were managed with [endoscopic retrograde cholangiopancreatography]. Even what’s considered early is quite variable, from 48 hours to anything less than six weeks,” Dr. Visser noted.
When surgeons do decide to delay repair, as Dr. Visser often does, he cautioned that they may face some challenges not necessarily seen in an early repair. “I tend to wait longer than six weeks out to two or three months; the injured duct retracts up, so you have to make a central hepatotomy to get access to the bile ducts. And you risk disrupting the collaterals you’ve been relying on to perfuse the right biliary tree in order to do your reconstruction,” he said.
If the right lobe has started to atrophy, with left-sided compensatory hypertrophy, “you may choose to do the right hepatectomy and a hepaticojejunostomy for a nicely perfused left bile duct,” he said, acknowledging that this can feel like subjecting the patient to increased morbidity.
“My takeaways? I think early repair is great for the subset of patients for whom everything lines up.” Dr. Visser said. “The five-day to six-week period is a no-go; longer than six weeks is probably better when you want to delay. This does come at a price to the patient and the healthcare system. But the principles of repair are the same whenever you do the repair.”
=This article is from the June 2025 print issue.
Please log in to post a comment