


Clinicians and health systems may find it easier to predict same-day surgical case cancellations using a newly designed prediction instrument.
The instrument can be applied preoperatively to a broad patient population and then be used to create and implement interventions to reduce same-day cancellations.
“The cancellation of scheduled operations on the day of surgery has several negative effects,” said Karuna Wongtangman, MD, the chief of the perioperative digital health laboratory in the Department of Anesthesiology at Montefiore Medical Center, in New York City. “Most importantly, patients don’t get their treatment and surgical services don’t get paid.
“While we know there are many factors that come into play with respect to same-day case cancellation, there is no prediction instrument that clinicians can use to forecast the risk of its occurrence,” she added.
To address this issue, Wongtangman and her colleagues—an interdisciplinary team composed of representatives from a broad range of hospital departments—turned to data in the institution’s electronic health record system for scheduled elective procedures performed at four campuses of the Montefiore health system (Moses, Einstein, Wakefield and Hutchinson) between January 2016 and June 2021. Procedures that were scheduled during the March to June 2020 COVID-19 surge were excluded from the analysis.

Factors Affecting Cancellations Identified
The study’s primary outcome was same-day case cancellation, which the researchers defined as the cancellation of a surgical procedure within 24 hours of its scheduled date and time. Data were analyzed for associations between case cancellation and a variety of potential patient, institutional and procedural characteristics (Table 1). These characteristics were included as independent variables in a multivariable logistic regression model.
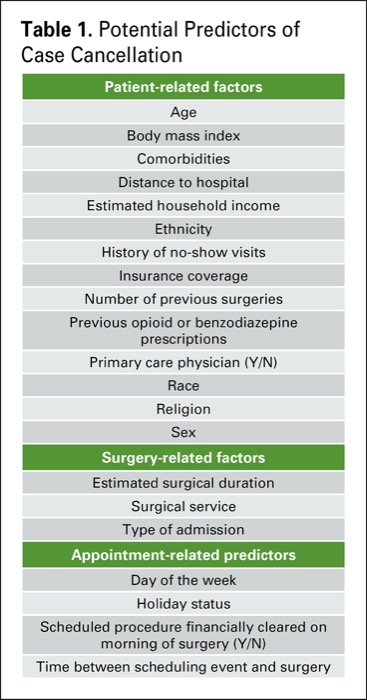
| Table 1. Potential Predictors of Case Cancellation |
| Patient-related factors |
|---|
| Age |
| Body mass index |
| Comorbidities |
| Distance to hospital |
| Estimated household income |
| Ethnicity |
| History of no-show visits |
| Insurance coverage |
| Number of previous surgeries |
| Previous opioid or benzodiazepine prescriptions |
| Primary care physician (Y/N) |
| Race |
| Religion |
| Sex |
| Surgery-related factors |
| Estimated surgical duration |
| Surgical service |
| Type of admission |
| Appointment-related predictors |
| Day of the week |
| Holiday status |
| Scheduled procedure financially cleared on morning of surgery (Y/N) |
| Time between scheduling event and surgery |
In a presentation at the 2022 virtual annual meeting of the International Anesthesia Research Society (abstract 1294), Wongtangman said 246,612 scheduled procedures were included in the analysis. Of those, 21,243 (8.6%) were canceled on the same day.
Multivariate regression analyses found 26 elements predicted same-day case cancellations, which were then incorporated into a predictive score model and weighted (Table 2), as follows:
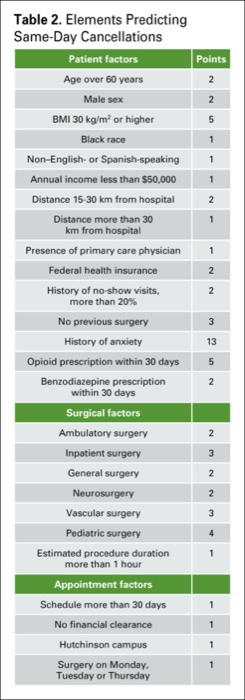
| Table 2. Elements Predicting Same–Day Cancellations | |
| Patient factors | Points |
|---|---|
| Age over 60 years | 2 |
| Male sex | 2 |
| BMI 30 kg/m2 or higher | 5 |
| Black race | 1 |
| Non–English- or Spanish-speaking | 1 |
| Annual income less than $50,000 | 1 |
| Distance 15-30 km from hospital | 2 |
| Distance more than 30 km from hospital | 1 |
| Presence of primary care physician | 1 |
| Federal health insurance | 2 |
| History of no-show visits, more than 20% | 2 |
| No previous surgery | 3 |
| History of anxiety | 13 |
| Opioid prescription within 30 days | 5 |
| Benzodiazepine prescription within 30 days | 2 |
| Surgical factors | |
| Ambulatory surgery | 2 |
| Inpatient surgery | 3 |
| General surgery | 2 |
| Neurosurgery | 2 |
| Vascular surgery | 3 |
| Pediatric surgery | 4 |
| Estimated procedure duration more than 1 hour | 1 |
| Appointment factors | |
| Schedule more than 30 days | 1 |
| No financial clearance | 1 |
| Hutchinson campus | 1 |
| Surgery on Monday, Tuesday or Thursday | 1 |
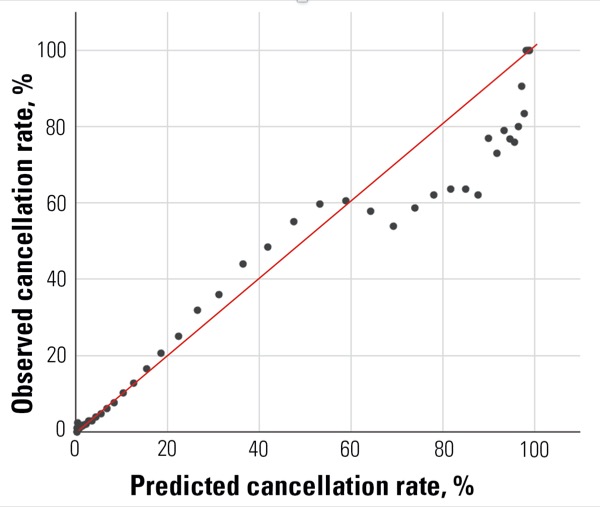
Using these variables, the researchers found a cutoff value of 16.5 points predicted a same-day case cancellation rate of 10.4% (Figure 1).

For example, if you schedule a 65-year-old, obese, non–English-speaking male with a history of anxiety for same-day surgery, he will have a score of 25 points, which has a predicted cancellation rate greater than 30%. “If you scheduled this patient for inpatient vascular surgery, this risk would increase to more than 50%,” Wongtangman added.
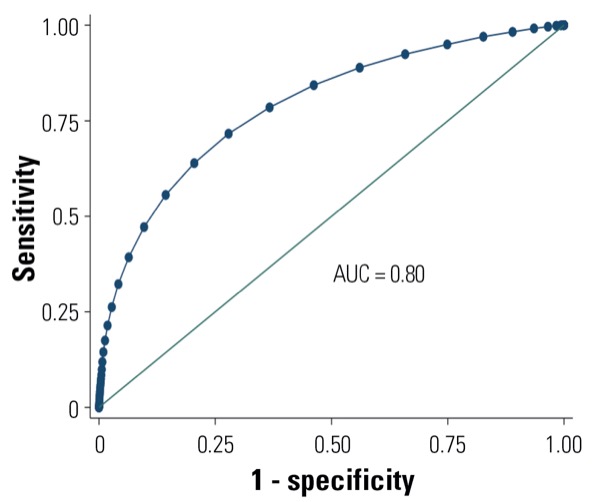
Using the cutoff threshold of 16.5 points, the score demonstrated what the researchers called “good” model discrimination, with a sensitivity of 0.67 and specificity of 0.77. In addition, the model aligned well with the observed same-day cancellation rate, yielding an area under the receiver operating characteristic curve (AUC) of 0.80 (95% CI, 0.79-0.80) (Figures 2 and 3). Similarly, when the researchers performed 30-fold cross-validation of the model, they found an AUC of 0.80 (95% CI, 0.79-0.80).
Hospital and OR Efficiency Is Key
Wongtangman’s team believes application of the prediction instrument may improve hospital operating efficiency.
“If a patient has a case cancellation risk of more than 25%, we will send them for a PAT [preadmission testing] visit,” Wongtangman explained. “Once there, we plan on enhancing engagement and education in certain individuals.”
As the study’s senior author Matthias Eikermann, MD, PhD, noted, development of the case cancellation tool is part of a larger effort aimed at personalizing Montefiore’s preadmission test visit.
“We want to add resources to our vulnerable patients who carry a high risk of case cancellation, for example due to an anxiety disease or inability to commute to the facility,” said Eikermann, the Francis F. Foldes Professor and chair of anesthesiology at the medical center. “We invest in additional patient engagement as well as in paid transportation to the facility.”
—Michael Vlessides
Eikermann and Wongtangman reported no relevant financial disclosures. The abstract was honored as one of the meeting’s best papers.
Please log in to post a comment