

SAN FRANCISCO—Continuing our coverage of the popular 10 Hot Topics in General Surgery, from the 2024 Clinical Congress of the American College of Surgeons, General Surgery News highlights the next two presentations from the session (for Part 1, see March 2025, page 1).
Endoscopic Treatment of Common Bile Duct Injuries

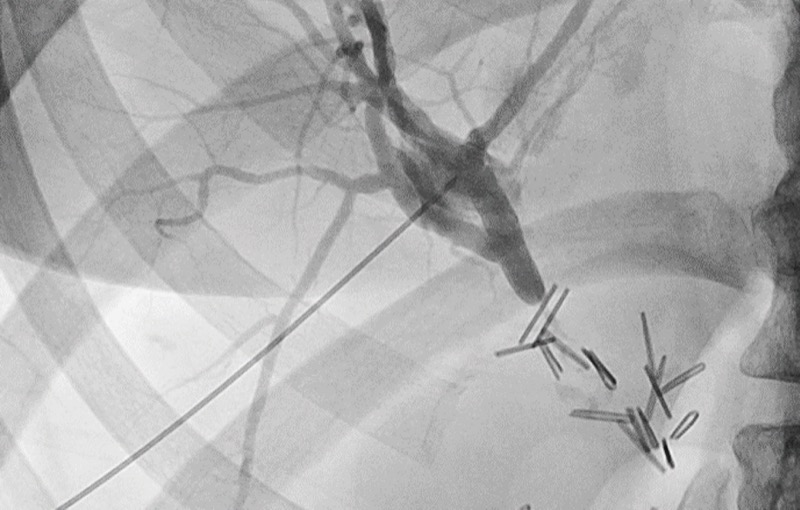
Gary C. Vitale, MD, a professor of surgery at the University of Louisville, in Kentucky, discussed the role of endoscopic treatment for common bile duct (CBD) injuries.
“The goals of endoscopic interventions are to reestablish biliary drainage, treat bile leaks, correct defects and try to normalize the anatomy,” he began, “and sometimes it’s a palliative approach until we can get around to surgery.” Typical endoscopic interventions include endoscopic retrograde cholangiopancreatography (ERCP), sphincterotomy, stenting and balloon dilatation.
Surgeons who choose candidates for endoscopic treatment need to make such decisions on an individual basis. For instance, septic patients tend to undergo open surgery, as do those who have undergone prior upper GI operations. Furthermore, the characteristics of the injury will affect whether an endoscopic approach is feasible. Such characteristics include the time from injury to presentation, the continuity of the bile duct, the bile leak condition (localized or generalized), and the length and location of the stricture or previous operative repair.
“Discovery of an injury early in the postoperative period improves options for endoscopic treatment,” Dr. Vitale noted. Gathering information about the anatomy is also helpful, including stricture length (<1 cm is optimal). In any case, continuity of the bile duct must be demonstrated for the procedure to work.
However, endoscopic interventions are not indicated in certain circumstances, including complete obstruction, inability to pass a guidewire, segmental loss of the bile duct, worsening peritonitis and/or prior gastric surgery.
Multiple series have looked at endoscopic treatment of benign strictures, including one performed by Dr. Vitale and his colleagues at the University of Louisville. Of 86 patients with such strictures, 78% were managed endoscopically, while 14% required surgical intervention and 8% had no surgery. The recurrence rate was 3%; complications occurred in 4.9% of patients; and procedure-related mortality was 0%.
“The procedure-related mortality appears to be very low,” he noted. “We do have deaths from pancreatitis with ERCP. They’re fortunately rare, but they do occur.”
Is there a role for chronic stenting in these patients? In most studies, stents need to be left in place for 12 to 16 months to cause strictures to remodel. ERCP is performed intermittently during that time to dilate the stricture and increase the number of stents. Usually one to three 10 Fr stents are used; these can be either plastic or metallic. Either way, long-term follow-up is critical regardless of whether patients have undergone endoscopic or surgical management, since both can have late stricture recurrence; some will likely need to be converted to surgery. Long-term stenting also may be more costly than a single operative procedure.
“When you’ve got a surgery that works, should we even be trying endoscopic management?” Dr. Vitale asked. “Well, with a 5% to 8% mortality rate with surgery, I certainly think trying endoscopy first makes sense, even in the complex strictures.”
Radiofrequency Ablation For Thyroid Nodules
Priya H. Dedhia, MD, PhD, an assistant professor of surgery at The Ohio State University Wexner Medical Center, in Columbus, discussed radiofrequency ablation (RFA) for thyroid nodules, which she said is becoming an increasingly popular treatment strategy.
“The majority of thyroid nodules are benign,” she began, “and there are multiple different causes. Ideally, we don’t need to perform operations.”
Most thyroid operations are performed for benign thyroid nodules, not malignant disease. Yet this can be an issue for patients because thyroidectomy comes with expected outcomes and complications that can affect their quality of life, including hypothyroidism. Less common postoperative complications include hematoma, decreased parathyroid activity and recurrent laryngeal nerve injury.
Given these possibilities, alternative strategies have been developed to address symptomatic thyroid nodules, including ethanol ablation, laser ablation, high-intensity focused ultrasound, microwave ablation and RFA. RFA involves the introduction of an alternating current in the tissue that ultimately leads to heat production, thereby forming tissue coagulation and tissue destruction through necrosis.
RFA is desirable because it offers superior volume reduction relative to laser ablation (approximately 70% at six months; 80% at three years). Dr. Dedhia said RFA also has lower risk, improved quality of life and better patient satisfaction compared with surgery. Its relatively low complication rate is another important reason to consider RFA, particularly when compared with microwave ablation. Among the several indications for RFA are compressive symptoms and cosmesis.

“In order to go ahead with RFA, usually we require two benign FNA [fine-needle aspiration] biopsies,” she noted.
RFA also can be performed for toxic nodules, although it is most effective when the nodules are less than 20 mL in volume. In addition, RFA is most effective in one large, predominantly solid nodule.
Treatment goals with RFA include a volume reduction ratio of 50% or greater, along with improvements in patients’ symptom and cosmetic scores.
General contraindications to RFA include contralateral vocal cord paralysis, pregnancy, presence of a pacemaker or defibrillator, and clotting/bleeding disorders. Specific contraindications include the presence of large bilateral nodules, nodules that are difficult to visualize and nodules with large cystic components. Data are evolving for the efficacy of RFA in indeterminate nodules and malignancies.
Unique considerations for RFA include using a trans-isthmic approach, which decreases the risk for complications. In addition, the “moving shot technique” prevents the delivery of high heat for prolonged periods in a single area.
The most common complication with RFA in patients with thyroid nodules is a temporary voice change (approximately 1.5%). Other less common complications include hematoma, skin burn and nodule rupture; hyperthyroidism, hypothyroidism, thyroiditis and brachial plexus injury are very rare.
This article is from the April 2025 print issue.
Please log in to post a comment