


An innovative technique of targeted blocking of the celiac ganglia during foregut surgery dramatically improves patient recovery time and outcomes, according to a recent study published in The Journal of Obesity Surgery (2025;35[6]:2101-2110). For Sunil K. Sharma, MD, the clinician who pioneered the approach, widespread implementation has the potential to revolutionize the way patients recover from these common upper abdominal surgical procedures.
“During the COVID pandemic, when hospitals were shut down and inpatient hospital surgery was disrupted, I began to think about how to develop a method that would allow more surgeries to be performed on outpatient basis,” said Dr. Sharma, chief surgeon at New Life Surgical Associates, in Jacksonville, Fla. “The key barrier we needed to address was better control over pain, nausea and vomiting after the surgery.
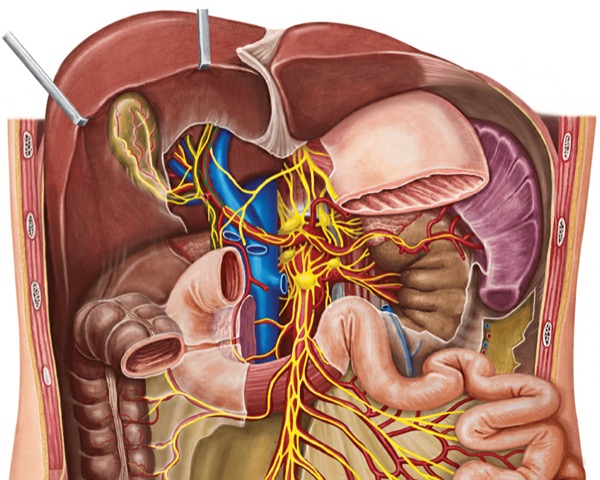
“And while we often address somatic pain effectively using local anesthesia and transversus abdominal plane blocks, visceral pain is traditionally ignored or treated with narcotics, which come with a host of adverse effects,” he continued. “In the case of foregut surgery, the sympathetic and parasympathetic nervous system is mediated through the celiac ganglia, which supplies the visceral sensory fibers to organs like the stomach, pancreas, liver and esophagus. So, I began to wonder if we can anesthetize or block this relay station, possibly stopping the visceral pain cycle.”
After trying several different drug combinations, Dr. Sharma landed on a cocktail comprising bupivacaine, dexamethasone and dexmedetomidine. He used this combination in the current study of 457 patients (81% female) undergoing outpatient laparoscopic metabolic and bariatric surgery at the ambulatory surgical center between January 2021 and July 2024 (43 years of age on average; average BMI, 38.4). The majority of participants (67%) underwent sleeve gastrectomy.
“Of course, there were issues when we first started performing the technique,” Dr. Sharma said in an interview with General Surgery News. “How do you expose the ganglia? What combination of drugs to inject? What’s the best way to inject the mixture? But now that I’ve mastered it, it takes only a few minutes to perform, and without the use of CT scan, fluoroscopy or x-ray, which are used in traditional approaches to the celiac ganglia.
“The block also reduces requirements of anesthetic gas and need of narcotics during surgery,” Dr. Sharma added. “And because we’re not using narcotics, patients are extubated much earlier, often before I even close the skin.”
When the researchers examined 30-day outcomes in this patient group, they found an exceedingly low number of adverse events, as follows:
- mortality, 0%;
- leak, 0%;
- bleeding, 0%;
- pulmonary embolism, 0%;
- unplanned return to the OR, 0.4%;
- unplanned readmission, 1.75%;
- transfer to hospital, 0%; and
- unplanned ICU admission, 0%.
These results, Dr. Sharma said, were appreciably superior to those reported in the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) 8th Global Registry Report in 2023, which noted a reoperation rate of 1.4%, a readmission rate of 2.7%, an ICU admission rate of 1.4% and a mortality rate of 0.04%.
The most dramatic improvement, however, was the change in postoperative length of stay. While patients in the IFSO registry averaged 55 hours in the hospital, Dr. Sharma’s patients went home after just 2.05 hours.
“The majority of my patients never required a narcotic,” he told GSN. “These patients are wide awake within 15 minutes of surgery, they walk in 20 to 30 minutes and they’re out of my center within two hours. And not a single one was transferred to the hospital for nausea, vomiting or the need for pain medication.”
Perhaps not surprisingly, patient satisfaction was extremely high, with an average score of 9.8 out of 10. This, Dr. Sharma said, was markedly higher than the traditional 7.2 satisfaction score among inpatients at his institution.
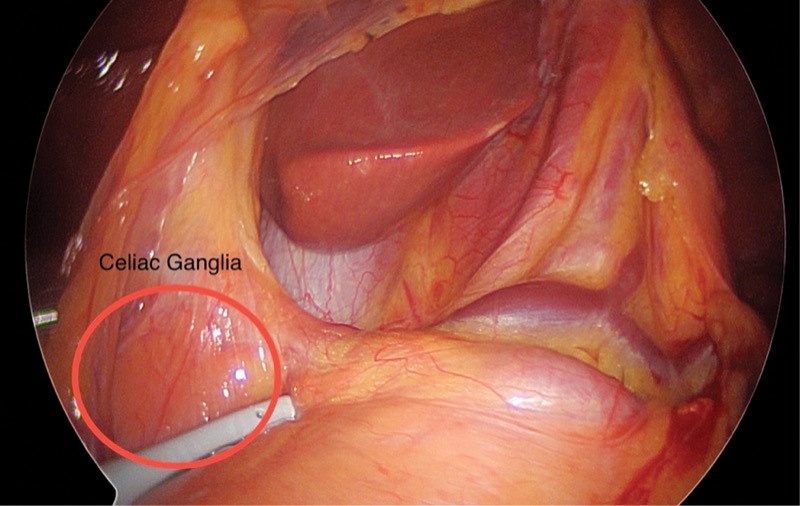
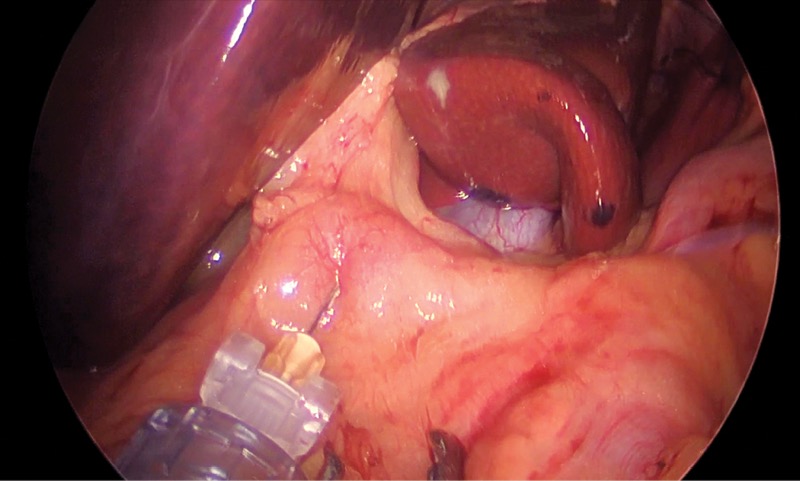
Dr. Sharma performs the block under general anesthesia. After standard port placement in the patient’s abdominal cavity, he incises the peritoneum close to the celiac trunk, where he exposes and identifies three to four ganglia. Using a dedicated probe, he injects 5 to 10 ml of the solution, depending on the size and number of ganglia.
“The ganglia are sitting on top of the aorta, so you have to be careful with the injection,” he said. “Many patients will experience a drop in blood pressure during surgery, so you have to make sure they’re well hydrated beforehand.
“But if a surgeon can perform foregut surgery, they can certainly expose and numb the ganglia … if shown how to do it properly.” This process will likely be facilitated in the future by a dedicated injection probe Dr. Sharma is currently developing.
As Dr. Sharma concluded, wider acceptance and implementation of the technique may offer significant benefits for physicians, institutions and, most importantly, patients.
“It saves money, it saves resources and patients can go home a couple of hours after surgery, which is where they want to recover,” he said. “Ultimately, I believe the block can be utilized in the majority of foregut surgeries. It dramatically cuts down the hospital stay, there are no narcotic-related side effects and no postoperative visits to the ER for dehydration or pain.
“And the only thing you need is to properly identify the ganglia and inject the fixed amount.”
For Michael Goldfarb, MD, a clinical professor of surgery at Rutgers New Jersey Medical School in New Brunswick, NJ, Dr. Sharma’s approach to the celiac ganglia has the potential to revolutionize the way patients recover from foregut operations.
“This is going to change surgery,” he said. “These are patients who undergo two or three hours of surgery, usually receive no opioids during the procedure and still go home a couple of hours later. The potential impacts on the entire healthcare system are profound.”
While Dr. Goldfarb recognized that the block “is not for beginners,” he said proper training and instruction should be enough to see most general surgeons performing the precise block in no time. And once patients hear about the procedure and its impact on recovery, Dr. Goldfarb said the proverbial floodgates will open.
“Things change in surgery for two reasons: Duration of surgery/recovery and patient demand,” he explained. “This hits on both levels.”
Physicians interested in learning more about the technique can contact Dr. Sharma at sharma@newlifejax.com. Drs. Goldfarb and Sharma reported no relevant conflicts of interest.
This article is from the August 2025 print issue.
Please log in to post a comment
I congratulate Dr. Sharma on his findings. However, the Obesity Surgery article by Dr. Sharma (Volume 35, Issue 6, pp. 2101–2110), which supports this GSN report, is actually titled “Safety of Same-Day Discharge Bariatric Surgery: A Comprehensive Analysis of 457 Cases”, with no mention of a “celiac block” in the title, abstract, or indexed keywords. The report is retrospective and uncontrolled, offering only descriptive observations; it cannot support the sweeping claims highlighted in the GSN article. Yet, in the GSN article, the author is credited with “novel celiac block” and dramatic improvements in recovery, PONV, visceral pain, and anesthedia consumption as well as the use of adjuncts to prolong bupivacaine effect, which is incongruent with what’s published in the peer-reviewed journal.
I want to point out that our group has extensively researched and published on autonomic neural blockade (ANB) in foregut (bariatric, paraesophageal, Nissen, and others) and other minimally invasive procedures, including colectomies, cholecystectomies, and hysterectomies. Over the past several years, we have published more than seven peer-reviewed articles in leading journals—JAMA Surgery, Surgical Endoscopy, Obesity Surgery, and right here in General Surgery News—in addition to textbook chapters and video demonstrations.
Most of the specific outcomes and formulations reported by the author closely resemble our results after extensive research. Still, no citation or acknowledgment is given to our publications detailing the ANB technique.
Here are some of our contributions: