


When Dana A. Telem, MD, MPH, and her colleagues at the Michigan Surgical Quality Collaborative set out to implement the Core Optimization Hernia Registry, or COHR, in 2020, they may not have foreseen the potential impact the registry could have on clinical care for people undergoing hernia surgery. Four years later, what started out as mere potential is turning into a reality that Dr. Telem believes may forever change the way surgeons communicate surgical risk to their patients, using the HerOIQ (Hernia Optimization for Improved Quality of Life) tool.
“The COHR registry [www.mcohr.org] is mirrored after the Danish Hernia Database, and aims to fill a gap,” said Dr. Telem, the Lazar J. Greenfield Professor of Surgery at the University of Michigan Health, in Ann Arbor. “The ACHQC [Abdominal Core Health Quality Collaborative] database is fantastic, but its surgeon-entered data may lead to selection bias, since the people who take the time to enter data are likely the ones most interested in quality improvement. What’s more, most of the patients in that database come from a small number of surgeons. So, I always look at that registry as the best possible outcomes of hernia disease.”
By comparison, COHR abstracts a variety of preoperative, intraoperative and patient-reported outcome data from 72 hospitals across Michigan. The database currently comprises approximately 20,000 patients from more than 700 unique surgeons. In 2022, COHR also added one-year follow-up data, which include insights into hernia recurrence and postoperative quality of life.
The COHR Lab, as it is known, seeks to improve hernia management in a variety of innovative ways for both patients and clinicians, including discovery, collaboration and quality improvement. But as Dr. Telem explained, the most significant product of COHR’s cutting-edge approach to healthcare improvement is the HerOIQ tool.
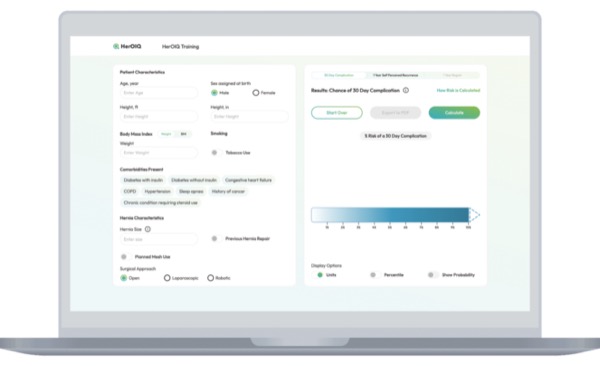
At its root, HerOIQ (herniacalc.com) is a hernia risk calculator designed to improve risk communication between surgeons and patients undergoing hernia repair. The tool uses patient-specific data, such as demographics, comorbidities, smoking status, and details about the hernia and planned repair to predict such risks as 30-day postoperative complications, self-perceived hernia recurrence after one year and patient regret within one year of surgery.
Using HerOIQ, surgeons can sit down with patients and talk about all these factors. The goal of the tool is to foster a dialogue between the clinician and patient.
“Often, we tell our patients things like ‘lose weight,’” Dr. Telem told General Surgery News. “But with HerOIQ you can actually show them their risk today, then change different variables to show them how it will impact their chance of recurrence. Then you can export it as a PDF or print it out and hand it to them. In the end, we’re trying to give people more granular information about why we’re telling them certain things.”
As Dr. Telem explained, by helping to cultivate a conversation between clinicians and patients about risk factors in surgery, HerOIQ also works as a springboard toward surgical optimization and prehabilitation. Chief among patient characteristics, she noted, are smoking and hemoglobin A1c levels, both of which can markedly harm postoperative outcomes. The website also incorporates a series of guidelines and other resources designed to help patients improve their preoperative physical status.
“Everything is there,” Dr. Telem said. “It’s really like a one-stop shop.”

Michael A. Rubyan, PhD, MPH, a clinical assistant professor of health management and policy at the University of Michigan School of Public Health, partnered with Dr. Telem to develop and design the HerOIQ tool. As he said, it’s the first that he knows of that can help facilitate nonjudgmental preoperative discussions about risk factors.
“I come from a public health background, where we often focus on how we communicate to the public,” Dr. Rubyan noted. “But as an implementation scientist, I wanted to make sure it could be easily incorporated into practice and used with patients. That’s why I think this has been a really fascinating partnership because it blends those two domains. To my knowledge, there hasn’t been a graphic tool like this that helps patients visualize risk and see how changes in behavior will modify that risk.”
For clinicians who may be daunted by the prospect of implementing yet another tool into their clinical armamentarium, the developers of HerOIQ have included a significant, easy-to-use training component, one they say has been optimized itself to maximize facility and the user experience.
“Our goal is to give people something useful in the context of training that’s palatable no matter how they like to be trained,” Dr. Telem noted.
In the end, a tool is only effective if it’s actually employed in practice, a reality that Dr. Telem and her colleagues recognize all too well. Fortunately, beta testing of the tool and its associated resources has yielded encouraging results.
“We’re so proud of this product and we think it could be so helpful,” she said. “But people need to know about it before they can use it. I’m happy to say that everyone who has been introduced to HerOIQ has incorporated it into their practice.
“I don’t share things until I have something to share,” Dr. Telem added. “But we believe in this work and we stand behind it. And the people who have used it have all been really excited about it.”
Dr. Rubyan agreed. “It’s easy to come up with a tool and just throw it out there. But it has to make sense. And I think the best part of HerOIQ has been just that—the response.”
Interested surgeons are encouraged to visit the HerOIQ website at herniacalc.com, create a user account and explore its various tools and resources.
Work for this project was funded through the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Rubyan reported that the HerOIQ platform was developed by Honey Locust Health, of which he is a partial owner. All development and evaluation performed by Dr. Rubyan was in his capacity as a University of Michigan investigator.
This article is from the February 2025 print issue.
Please log in to post a comment