


A panel of 15 colorectal surgeons compiled a set of recommendations for how to prevent surgical site infections, based on their expert opinion and review of dozens of studies.
The recommendations include advice on what to use, what lacks sufficient evidence to support its use, and nuanced approaches to wound irrigation and the location of incisions (J Am Coll Surg 2022;234[1]:1-11).
According to a 2020 study, 23.9% of patients develop an ssI after colorectal cancer surgery, which can cost commercial payors up to $145,000, and $102,000 to Medicare within a year (Dis Colon Rectum 2020;63[12]:1628-1638).
The goal is to reduce the burden of SSIs, said senior author Traci Hedrick, MD, FACS, FACRS, a colorectal surgeon at the University of Virginia Health System, in Charlottesville.

“Most of these recommendations are on topics that surgeons are already familiar with,” Dr. Hedrick said. “However, the intraoperative aspects can sometimes get lost in the large comprehensive bundles, which is why this project is unique.”
To prevent SSIs, the authors suggest surgeons employ wound protectors/retractors, negative pressure wound therapy, triclosan-coated sutures, a sterile incision closure tray and change their gloves before closing the incision. Alternatively, they found that there was insufficient evidence to recommend topical skin adhesives, incise/adhesive drapes, advanced dressings, continuous versus interrupted sutures or staples, a delayed incision closure, and subcutaneous drains to specifically prevent SSIs (Figure).
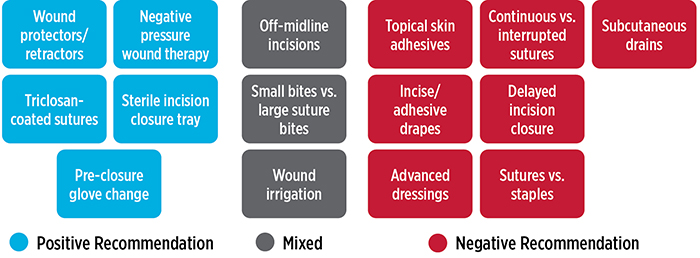
With some topics, the advice was more complex—not a simple do or don’t do, Dr. Hedrick said. For instance, when it comes to midline incisions, the panel determined there was insufficient evidence that off-midline incisions reduce the risk for SSIs compared with midline incisions, but when possible and appropriate, off-midline incisions may reduce incisional hernia risk after (laparoscopic) colorectal surgery. With the size of bite sutures, the authors said there was not enough evidence to conclude that a small bites suture technique does more to reduce ssI risk than a large bites suture technique. However, they said the small bites suture technique can reduce the risk for incisional hernias. Regarding wound irrigation, use aqueous iodine, not antibiotic incisional wound irrigation, in high-risk, contaminated wounds.
To reach a consensus, the panel followed a modified Delphi method, with up to three rounds of discussion for each topic. Voting was anonymous, as is “standard” in this type of process, Dr. Hedrick said, so voters aren’t influenced by their peers. Every recommendation had to reach at least 70% agreement among voters. “We reviewed each of the topics with a fine-toothed comb and did a thorough review of all the evidence,” she said. “We took our time resolving each of the recommendations.”
The report offers practical advice to help surgeons prevent one of the most common, and costly, complications following colorectal procedures, said Syed Husain, MD, FACS, FASCRS, a colorectal and general surgeon at The Ohio State University, in Columbus, who did not participate in the study. “These are the questions that we grapple with on a daily basis, and the authors have gone really to the heart of the problem.”
The result of these discussions by the expert panel in the report is extremely helpful to practicing surgeons, Dr. Husain said. For instance, his practice frequently uses glue sealants on top of incisions. Although he and his colleagues haven’t stopped yet, these recommendations have “definitely started a conversation in our group.” If they don’t stop entirely, they may begin to employ glue sealants more selectively, he added. “There’s a very good chance that we’re going to move away from the blanket application in all patients.”
His practice also doesn’t usually have access to antibiotic-impregnanted sutures. But after the panel recommended their use to prevent SSIs, “that has again started a conversation in our group and administration to have those available to us.”
It can be hard to determine how best to prevent SSIs, Dr. Husain said, because doctors can’t easily try something to see what works. In the future, the surgical community will hopefully find a way to conduct randomized, prospective trials of techniques to reduce ssI risk in a way that won’t compromise patient care, he added.
Disclosures: Dr. Hedrick is a consultant to Ethicon/Johnson and Johnson, which provided funding for the study. Dr. Husain reported no relevant financial disclosures.
This article is from the April 2022 print issue.
Please log in to post a comment