

ORLANDO, Fla.—Granulomatous mastitis, an uncommon, inflammatory benign breast disease, can be frustratingly hard to treat. But a recently developed algorithm based on the findings of an American Society of Breast Surgeons (ASBrS) registry study might provide physicians with some guidance.
“Since there are no clear management guidelines for granulomatous mastitis [GM], it has become a frequent topic of discussion on our member forums,” said Nimmi Kapoor, MD, a breast surgical oncologist and an associate professor of surgery at the David Geffen School of Medicine at the University of California, Los Angeles.
To address this uncertainty and lack of guidance, Dr. Kapoor and her colleagues designed a prospective, multiple-site registry with data entered by ASBrS members recording the presentation of GM, incidence of relapse and time to resolution of symptoms.
“The primary aim of this study was to identify treatment strategies that result in the shortest duration of symptoms as well as the optimal cosmesis,” Dr. Kapoor said, presenting her research at the 2024 annual meeting of the ASBrS.
Registry data included patient demographics, with initial symptom severity considered mild if it involved less than 10% of the breast, moderate if it involved up to 25%, and severe if more than 25%. Medical intervention included nonsteroidal anti-inflammatory drugs (NSAIDs), antibiotics, oral steroids and intralesional steroid (ILS) injection. Surgical intervention included aspiration, incision and drainage, and excision.
“Follow-up was done at one, three, six and 12 months to capture changes in treatment, symptoms and cosmesis over the course of the registry,” Dr. Kapoor said.
The study included data on 112 patients entered by 45 surgeons. The patients’ mean age was 36 years, and most were Hispanic or white.
Most patients (47%) had moderate symptoms, and the rest were evenly divided into mild or severe symptoms at presentation; 70% had medical treatment alone, 5% underwent surgical treatment, 20% had a combination of treatments and 5% had observation; and 83 (74%) had immunosuppressive therapy, 43 of them with ILS.
“A quarter of the patients had relapsing symptoms over the time course and 58% underwent a change in treatment,” Dr. Kapoor said.
Surgical intervention was more likely in patients with severe symptoms. At one month, 30 patients (26%) had experienced improvement or resolution without relapse, with one-month improvement/resolution being associated with immunosuppressive therapy. Two-thirds of those patients had medical intervention alone, and eight received ILS. At one year, 75% of patients had experienced improvement or resolution within a median of three months.
“On logistic regression, combination medical and surgical treatment was found to be more predictive of one-year improvement or resolution,” Dr. Kapoor said.
Data on one-year cosmesis were available for 35 patients, of whom 57% had excellent or good cosmetic outcomes, regardless of whether they presented with severe symptoms or had surgery. Excellent or good cosmesis ratings were, however, more likely in patients who experienced improvement or resolution within the year.
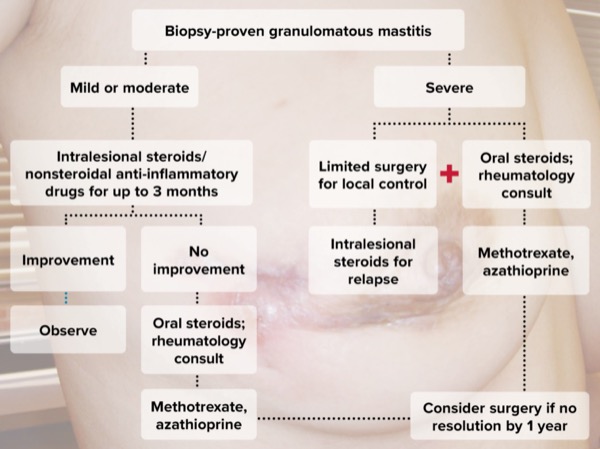
Given these findings, Dr. Kapoor and her colleagues recommend the following algorithm for biopsy-proven GM based on symptom severity (Figure):
- For patients with mild or moderate symptoms, they recommend a course of ILS and NSAIDs for up to three months as needed. “If there is no improvement or a relapse of symptoms, we recommend a change in therapy and consideration of oral steroids and a rheumatology consultation as needed. If at one year there are still persistent symptoms, we recommend consideration for surgical management.”
- In patients with more severe symptoms for whom ILS is insufficient, they recognize the importance of considering limited surgical intervention up front—drainage or limited excision. “At the same time, we recommend also starting oral steroids. Similarly, if by one year there is still no resolution, we recommend considering surgical intervention again.”
Theresa Schwartz, MD, a breast cancer surgeon with the Henry Ford Cancer Institute, in Detroit, considers GM one of the most vexing benign diseases breast surgeons manage, partly due to its lack of a known etiology. “We don’t know what causes it. There are theories that it’s caused by immune system–related inflammation, or that it’s a bacterial infection or a virus. We really don’t know where to start to get it to respond, and if you talk to 10 different surgeons, you won’t see the same treatment plan twice.”
Another challenge is that it’s so rare, most surgeons see only a few cases a year, she said. But those patients often require a disproportionate amount of care before finding resolution. “There aren’t many of them, but there are definitely GM patients I see more often than cancer patients for follow-up,” Dr. Schwartz noted.
She appreciated that Dr. Kapoor’s registry study included ASBrS surgeons who entered their own patient data, and that it included the majority of known treatments for GM. “It explains that we usually wouldn’t want to start with surgery, which immunosuppressant drugs to start with, and how to follow the treatment algorithm to get the best benefit.”
Dr. Schwartz hopes the algorithm will lead to more uniform treatment plans. “I think it would be a huge help. I was on a meeting yesterday with three others and all four of us treated it differently. Every one of us had a different way to start treatment.”
This article is from the November 2024 print issue.
Please log in to post a comment