

CLEARWATER BEACH, Fla.—Use of a prehabilitation protocol that emphasizes restoring good nutritional status and increasing exercise tolerance may help improve outcomes in patients undergoing surgery for enterocutaneous fistula, according to a new study.
As she was preparing her presentation for the 2024 Southeastern Surgical Congress, Lucie B. Moore, MD, now an ophthalmology resident at The Ohio State University, in Columbus, found high mortality rates of around 30% among patients with enterocutaneous fistulas. One 2023 paper reported a mortality rate of 38%.
“Whether it’s 30% or 38%, that’s very high, and management can be very complex because [these fistulas] are such a dangerous problem,” Dr. Moore said.
To address this problem, the University of Florida in Gainesville adopted a protocol—the University of Florida Abdominal Wall Reconstruction and Intestinal Rehab (UFAIR) service—in 2017, the outcomes of which have been recorded by the Fistula Registry at the university.

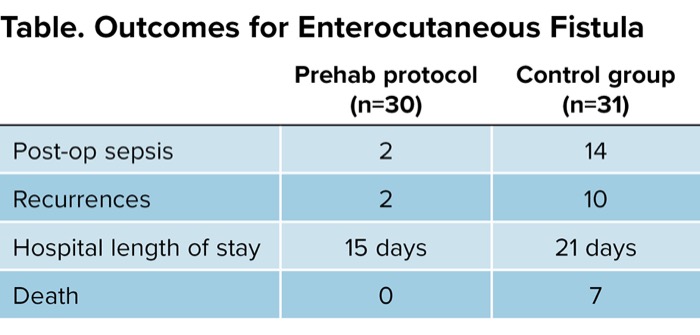
| Table. Outcomes for Enterocutaneous Fistula | ||
| Prehab protocol (n=30) | Control group (n=31) | |
|---|---|---|
| Post-op sepsis | 2 | 14 |
| Recurrences | 2 | 10 |
| Hospital length of stay | 15 days | 21 days |
| Death | 0 | 7 |
“Most would agree for management of fistulas early on, we need to get source control, to have electrolyte balance, to protect the skin from becoming macerated and to provide nutritional support, especially meeting caloric goals. This will help patients get ready to go to surgery. The UFAIR service is really dedicated to optimizing patients before taking them to surgery,” Dr. Moore said.
The UFAIR service focuses on an oral diet, when possible, in patients with a fistula of less than 1,000 cc per 24 hours output. “This is an increase from previous guidelines of 500 cc, so we’re being pretty diligent and aggressive with oral toleration of diet,” Dr. Moore said. When output is more than 1,000 cc per 24 hours, the team will rely on supplemental parenteral nutrition and watch for acute kidney injury caused by dehydration.
“Speaking of dehydration, we recommend our patients drink something close to the World Health Organization’s cholera solution. You need salt and sugar to absorb water into your GI tract,” she said.
The goal of physiotherapy is an hour daily on the treadmill at a grade 4 incline (about a 2.3-degree angle) at a speed of 4 miles per hour, followed by a 20-g protein load, to be synergistic with the exercise paradigm. Dr. Moore acknowledged that this can be a rigorous endeavor for a person with a fistula.
“I have a hard time doing that. But we collaborate with physical therapy and set up outpatient appointments with them to set goals and see that this is what we need them to do. Obviously, we can’t ensure 100% adherence to that, and it’s really hard when someone has a high-output fistula, but we’ll put a colostomy bag on them and try as well as we can to get them up and moving.”
Other prehabilitation goals include reducing excess body weight, controlling hemoglobin A1c and smoking cessation. A unique component of the service is the inclusion of nutrition shakes twice daily for a week before surgery. “We use Ensure [Abbott] shakes with arginine and omega-3 fatty acids to help with recovery,” Dr. Moore said.
To evaluate the effectiveness of the UFAIR service, Dr. Moore and her colleagues reviewed five years of protocol data from 61 patients: 30 in the intervention group and 31 controls. The primary outcomes were hospital length of stay, recurrences, readmission rates and mortality.
The two groups were similar in terms of age, race, fistula location and etiology, and Charleston Comorbidity Index score. Patients in the UFAIR group had significantly lower postoperative sepsis at two of 30 compared with 14 of 31 controls. “We had two recurrences in the UFAIR group compared with 10 in the control group, 15 days length of stay compared with 21, and no deaths compared with seven [in the control group],” Dr. Moore said.
Why do patients in the UFAIR group fare better? “We’ve done the logistic regression and we know that UFAIR patients are not inherently less sick than the control group. We believe it’s just a multidisciplinary approach addressing a multifactorial problem,” she said.
Jason Clark, MD, the director of the general surgeon residency at HCA Healthcare/Mercer University School of Medicine, in Charleston, S.C., commended Dr. Moore and her colleagues for championing this research. “Gastrointestinal fistulas are one of the most feared complications for any surgeon. As the authors have noted, treatment of this disease is complex, time-consuming, very costly, and carries high morbidity and mortality.”
He also appreciated the authors’ describing an approach to enterocutaneous fistula management that incorporates aspects of enhanced recovery after surgery (ERAS) protocols. “To date, there are many papers that discuss ERAS, but only one that I’m aware of that discusses ERAS and fistulas specifically.”
However, Dr. Clark noted that since ERAS was first discussed in 2005, guidelines have evolved over the years to incorporate up-to-date evidence. “How often do you reevaluate the literature to forge this modern, evidence-based approach?”
Dr. Moore said she and her colleagues are constantly on the lookout for new developments, and she meets with lead investigator Dr. Martin Rosenthal at least once a month to discuss the paper’s status and whether more recent data have been published.
This article is from the November 2024 print issue.
Please log in to post a comment