


It’s been on somewhat of a hiatus, but we are back and looking forward to 2023! In this installment of Journal Watch, we welcome guest columnist Kathryn Atkins, MD, MPH, who is a general surgery resident and current research fellow at the University of North Carolina at Chapel Hill School of Medicine. She takes a closer look at recent articles evaluating perioperative antibiotic use for choledocholithiasis, use of whole blood for resuscitation, recurrent laryngeal nerve monitoring during thyroidectomy and the creation of a statewide surgical collaborative to improve reexcision rates during breast-conserving surgery. We hope our readers will find these initial reviews worthwhile and relevant to the scope of a general surgeon’s practice.


University of North Carolina at Chapel Hill School of Medicine
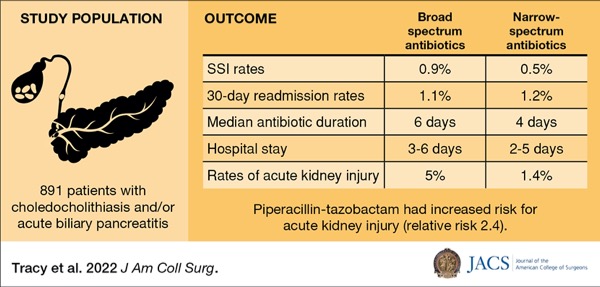
Broad- Versus Narrow-Spectrum Antibiotics in Common Bile Duct Stones: A Post Hoc Analysis of an Eastern Association for the Surgery Of Trauma Multicenter Study
In the Journal of the American College of Surgeons, Tracy et al presented a prospective, observational, multicenter study, conducted in the United States, examining the effect of broad-spectrum (BS) versus narrow-spectrum (NS) antibiotics on surgical site infections in patients with common bile duct stones undergoing same-admission cholecystectomy (2022;235[3]:411-419). The primary outcome was incidence of ssIs, while secondary outcomes included hospital length of stay (LOS), acute kidney injury rates and 30-day readmission rates for ssIs.
The study included 891 adults (=17 years of age) across 12 academic medical centers with choledocholithiasis and/or acute biliary pancreatitis, treated from 2016 to 2019. Patients presenting with acute cholangitis and nonbiliary infections, operatively confirmed gallbladder perforations, and prehospital biliary instrumentation were excluded. Patients were stratified by use of BS (51.7%) versus NS (48.3%) antibiotics. Patients receiving BS antibiotics were older, more likely to be male and had more comorbidities compared with the NS cohort. The BS cohort was more likely to have choledocholithiasis, cholecystitis and undergo preoperative endoscopic retrograde cholangiopancreatography (63.6% vs. 36.4%; P<0.001) compared with the NS cohort. First- and second-generation cephalosporins were the most commonly used antibiotics in the NS group, at 59.8% and 36.7%, respectively, whereas piperacillin-tazobactam (59.4%) and fluoroquinolones (23.4%) were most often used in the BS cohort.
No difference was found in the rates of ssIs (0.9% vs. 0.5%; P=0.7) or 30-day readmission rates (1.1 vs. 1.2; P=1.0) when comparing BS with NS antibiotic use. Median antibiotic duration was longer in patients receiving BS antibiotics (six [four to nine] vs. four [three to five] days; P=0.01), and hospital stay was generally longer in these patients (three to six days vs. two to five days; P<0.001). Rates of acute kidney injury were higher in patients who received BS antibiotics compared with those receiving NS antibiotics (5% vs. 1.4%; P=0.001), with an adjusted odds ratio (OR) of 2.8 (95% CI, 1.16-7.82; P=0.02) after controlling for antibiotic type, sex, cholecystitis and patient comorbidities. Further, piperacillin-tazobactam demonstrated an increased risk for acute kidney injury (relative risk [RR], 2.4; 95% CI, 1.18-4.92; P=0.02).
This is the first prospective, multicenter study to evaluate perioperative antibiotic use in patients with common bile duct stones and highlight the importance of antibiotic selection in this population. The study was limited by sample size; however, the multicenter nature improves external validity and applicability to the general population. The severity of gallbladder disease and intraoperative bile spillage was not documented, nor were patients excluded who developed hospital-associated infections (ventilator-associated pneumonia, catheter-associated urinary tract infection, etc.), which may have increased BS antibiotic use, hospital LOS and complications such as acute kidney injury.
Given this study found no difference in the ssI and 30-day ssI rates based on antibiotic selection, surgeons should consider administering NS antibiotics to patients with common bile duct stones undergoing same-admission cholecystectomy. This practice may decrease duration of antibiotic use, hospital LOS and rates of kidney injury in this population.
Use of Cold-Stored Whole Blood Is Associated With Improved Mortality In Hemostatic Resuscitation of Major Bleeding
In Annals of Surgery, Hazelton et al presented a prospective, observational, multicenter study in the United States, evaluating the use of cold-stored whole blood (WB) compared with traditional blood component therapy (BCT) during initial trauma resuscitation (2022;276[4]:579-588). The primary outcome was in-hospital mortality. Secondary outcomes included acute kidney injury, deep vein thrombosis, pulmonary embolism, pulmonary complications and bleeding complications.
All trauma patients who received any blood products while being managed in the emergency department (n=1,623) were included across 14 trauma centers, from 2016 to 2021. The study comprised primarily male patients (83%) with an average age of 35 years (interquartile range, 24-35 years of age), with 53% sustaining penetrating traumatic injuries. The patients were stratified by use of WB+BCT (73%) versus BCT alone (27%).
The WB cohort was older, more often male, with more comorbidities and more likely to have sustained blunt traumatic injuries compared with those who received BCT. Shock index (0.98 vs. 0.83; P=0.0001) and total Glasgow Coma Scale scores were higher in patients who received WB compared with BCT (14 vs. 10, respectively; P=0.004). There was no notable difference in Injury Severity Score indexes between the groups (22 vs. 21; P=0.33). Patients who received WB had higher hemoglobin levels initially and at 24 hours and lower platelets at four hours compared with the BCT cohort. Patients in the BCT cohort were transfused more packed red blood cells at four hours and within 24 hours compared with WB patients. There was no difference in the number of patients requiring massive and ultra-massive transfusion protocols between the groups.
After controlling for age, sex, prehospital blood administration, mechanism of injury and Injury Severity Score indexes, patients who received WB demonstrated a 9% reduction in bleeding complications (OR, 0.91; 95% CI, 0.91-0.91; P<0.001) and a 48% reduction in in-hospital mortality (OR, 0.52; 95% CI, 0.39-0.70; P<0.0001) compared with BCT alone. No differences were noted in the rates of acute care injury, deep vein thrombosis, pulmonary embolism or other pulmonary complications.
This is the first prospective, multicenter, observational study to evaluate cold-stored WB in trauma resuscitation in civilians. Prior studies have been primarily military use of warm WB in trauma resuscitation. This study is limited by the inability to assess dose-dependent complications, given that the majority of patients in the WB cohort received only one to two units. Further limitations of this study included the lack of standardized protocols for WB administration among the 14 institutions involved and the use of various blood banks supplying different types (plus/minus leukoreduction) and different titer levels of WB.
Hazelton et al demonstrated a 9% reduction in bleeding complications and 48% reduction in mortality in civilian trauma patients utilizing cold-stored WB in conjunction with BCT in trauma resuscitation, suggesting cold-stored WB may be beneficial in this population.
Effect of Intraoperative Neuromonitoring on the Risk for Recurrent Laryngeal Nerve Injury During Thyroidectomy: A Doubly Robust Approach
In Annals of Surgery, Memeh et al performed a retrospective review of a pooled data set, combining the National Surgical Quality Improvement Project (NSQIP) General Participant User File with the corresponding Targeted-Thyroidectomy file, to evaluate the relationship between intraoperative neuromonitoring (IONM) and recurrent laryngeal nerve (RLN) injury, given the ongoing controversial use during thyroidectomies (2022;276[4]:684-693).
The study included 24,370 patients (aged =18 years) who underwent thyroidectomy from 2016 to 2019. IONM was the exposure of interest with the primary outcome of RLN injury, characterized by voice hoarseness or vocal cord injury. Operative time and postoperative LOS were secondary outcomes. The authors used a doubly robust estimator—an inverse probability-weighted regression-adjustment model—to improve model misspecification, given the rare outcome of RLN injury.
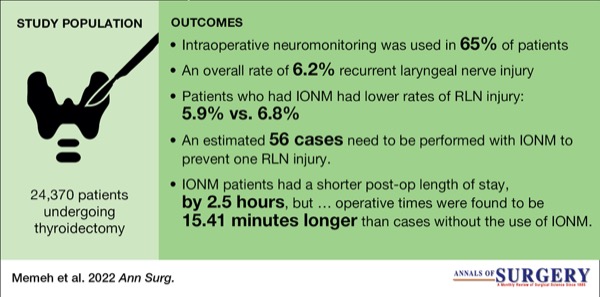
IONM was used in 65% of patients, with an overall 6.2% RLN injury rate in the study. IONM was more often used in patients who were Hispanic, American Indian, obese, those with prior neck operations, benign thyroid disease and those requiring a vessel-sealant device. Patients who had IONM experienced lower rates of RLN injury compared with those who did not (5.9% vs. 6.8%, respectively). Adjusted regression models demonstrated a 23% reduction in the rate of RLN injury (RR, 0.77; 95% CI, 0.68-0.87; P<0.001), estimating that 56 cases need to be performed with IONM to prevent one RLN injury. Further, IONM was associated with a shorter postoperative LOS by 2.5 hours (95% CI, –4.18 to –0.81 hours); however, operative times were found to be 15.41 minutes longer than cases without the use of IONM (95% CI, 13.29-17.54 minutes).
The large national data set produces unavoidable limitations. Coding of RLN injury is not well defined in the NSQIP database, separated only by levels of hoarseness, limiting delineation between hoarseness due to intubation, an injured nerve or if the injury is transient versus permanent. Further, the database does not provide information on hospital or surgeon volume of thyroidectomies, a known association with RLN injury. Presumably, as a national database this encompasses a range of surgeons with varying surgical volumes, thus making the results more generalizable.
This study is the largest of its kind to date, utilizing a national outcomes database to assess the effect of IONM on RLN injury, and shows a potential association between use of IONM and a reduction in RLN injury.
A Statewide Approach to Reducing Reexcision Rates for Women With Breast-Conserving Surgery
In Annals of Surgery, Schumacher et al presented a statewide evaluation of reexcision rates after breast-conserving surgery (BCS) for breast cancer following the Surgical Collaborative of Wisconsin (SCW) implementation of evidence-based strategies, utilizing existing discharge data and benchmarked performance reports (2022;276[4]:665-672). The SCW encompasses 85 hospitals and 224 surgeons and quality leaders throughout the state.
The SCW breast quality improvement initiative encompassed benchmarked performance reporting, a collaborative learning environment and education of evidence-based best practices. The Wisconsin Hospital Association hospital discharge database was used from 2017 to 2019 to provide participating surgeons with confidential, de-identified performance reports containing risk-adjusted and reliability-adjusted surgeon and hospital 60-day reexcision and mastectomy rates at baseline and to analyze post-initiative results. SCW surgeons were provided opportunities to gather and learn five times over the course of the study, attend two educational presentations and receive educational materials.
Patients were all women, 18 years of age or older, diagnosed with nonmetastatic breast cancer at the time of their index breast procedure. The primary outcome was 60-day reexcision rates after BCS. Mastectomy rates were evaluated as a secondary outcome to determine whether the intervention had a negative effect on mastectomy rates over time.
Over the baseline period in 2017, 3,692 patients underwent BCS at 63 SCW-participating hospitals (PHs), and 1,279 patients were treated at 54 nonparticipating hospitals (NPHs). At baseline, patients at SCW-PHs were younger and more likely to have insurance than those at NPHs. SCW-PHs had significantly higher breast surgery volumes at baseline (58.6 cases [SD, 77.1] vs. 23.7 cases [SD, 38.6]; P<0.01). Over the study period, 64.4% of SCW-PHs participated in one activity, with rates of 16.9% and 18.6% participating in two to three activities and four or more activities, respectively.
The study found no statistically significant difference in 60-day reexcision rates between SCW-PHs and NPHs at baseline (16.1% vs. 17.1%; P=0.46). A significant decrease in reexcision rates was demonstrated in the post-intervention period from 2018 to 2019 for SCW-PHs compared with NPHs (13.9% vs. 18.2%; P<0.001). Following adjustment for patient age, insurance status and baseline breast procedural volume, SCW-PHs demonstrated an OR of 0.69 for reexcision rates compared with NPHs (95% CI, 0.52-0.91; P=0.008). No significant difference in mastectomy rates was noted at baseline between SCW-PHs and NPHs (29.8% vs. 31.0%; P=0.43) as well as after intervention and adjustment (OR, 1.28; 95% CI, 0.93-1.78; P=0.13).
The database has an inherent limitation since it does not contain information about cancer diagnosis or treatment factors of individual patients to compare outcomes. Although demographics and baseline characteristics of patients and hospitals from 2017 are provided, this information is not specified for the post-intervention group. This information would be helpful to evaluate the number of patients treated, hospital case volumes and pertinent demographics, but these variables were controlled for within the adjusted analysis.
This study is the first with a statewide implementation initiative to address reexcision rates after BCS. An associated reduction in reexcision rates following thoughtful and evidence-based performance evaluation and education through a statewide collaborative may serve as an important model for other statewide collaborations to initiate similar quality improvement studies.
This article is from the February 2023 print issue.
Please log in to post a comment