The utility of aggressive intraoperative warming during noncardiac surgery has been called into question by the PROTECT trial.
The groundbreaking study (Lancet 2022;399[10337]:1799-1808)—which included more than 5,000 patients, over five times more than any previous perioperative thermal management trial to date—found that the incidence of a 30-day composite of major cardiovascular outcomes did not differ between patients randomized to routine care (35.5° C) and those who underwent aggressive warming (37° C). As such, the multicenter team of researchers concluded that keeping core temperatures at least 35.5° C in adult noncardiac surgical patients appears sufficient in this patient population.
“There have been previous small studies, mostly dating back two decades, that showed that hypothermia promotes surgical site infection, blood loss and transfusion requirements,” said Daniel I. Sessler, MD, the Michael Cudahy Professor and Chair of the Department of Outcomes Research at Cleveland Clinic. “But whether aggressive warming to a truly normothermic temperature, near 37° C, improves outcomes remains unknown.”
Pre-warming
Dr. Sessler and his colleagues enrolled 5,056 patients (aged =45 years) into the multicenter, parallel-group, superiority trial, all of whom underwent noncardiac surgery at one of 12 sites in China or Cleveland Clinic between March 27, 2017, and March 16, 2021. Patients were randomly assigned to either aggressive warming to a target core temperature of 37° C or routine thermal management to 35.5° C during surgery.
The participants all had at least one cardiovascular risk factor, were scheduled for inpatient noncardiac surgery expected to last between two and six hours under general anesthesia, and were expected to have at least half of their anterior skin surface available for warming.
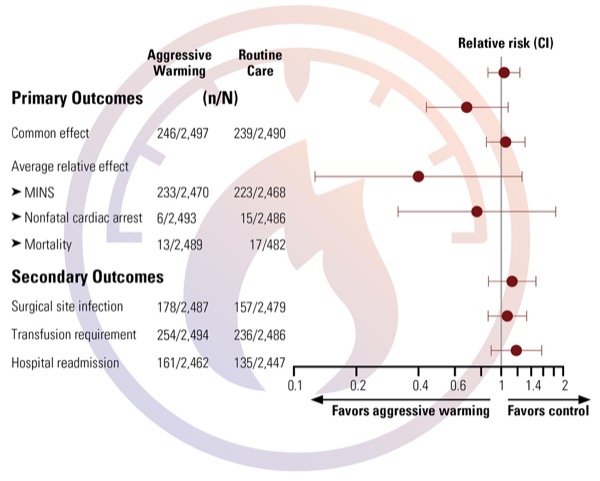
The study’s primary end point was a composite of myocardial injury (troponin elevation, apparently of ischemic origin), nonfatal cardiac arrest and all-cause mortality within 30 days of surgery.
Secondary outcomes included deep or organ-space surgical site infection within 30 days of surgery; intraoperative transfusion requirements; hospital length of stay; and hospital readmission within 30 days of surgery.
Dr. Sessler and his colleagues reported that 5,013 patients were included in the intention-to-treat population. Of these, 2,507 were aggressively warmed, while the remaining 2,506 underwent routine thermal management. Individuals assigned to the routine thermal management group did not have pre-warming, and ambient intraoperative temperature was maintained near 20° C; only transfused blood was warmed. If patients’ core temperature decreased to 35.5° C, warming ensued with an upper- or lower-body forced-air cover over a nonoperative site.
Patients in the aggressive warming group were pre-warmed with a full-body forced-air cover for approximately 30 minutes before anesthesia induction. These individuals were also aggressively warmed with two forced-air covers (when clinically practical) during surgery to a target intraoperative core temperature of at least 37° C. In addition, all IV fluids were warmed to body temperature and ambient intraoperative temperature was maintained near 20° C.
Patients who were assigned to aggressive warming had a mean final intraoperative core temperature of 37.1° C, compared with 35.6° C among their routine warming counterparts.
Results Not Underpowered
The study found that at least one of the primary outcome components (myocardial injury after noncardiac surgery, cardiac arrest or mortality) occurred in 9.9% (n=246) of 2,497 patients in the aggressively warmed group, compared with 9.6% (n=239) of 2,490 patients in the routine thermal management group (Figure). As such, the relative risk of aggressive versus routine thermal management was an estimated 1.04 (95% CI, 0.87-1.24; P=0.69).
“The results of PROTECT are ‘negative,’ but they are not underpowered,” Dr. Sessler said in an interview. “This is clearly a robust, equivocal outcome with small confidence intervals. The results are highly reliable.”
The trial found that the 30-day incidence of deep or organ-space surgical site infection, red blood cell transfusions and 30-day readmissions also did not differ between the two groups. Similarly, the median hospital length of stay did not differ significantly.
“I am not at all surprised with our findings on myocardial injury,” Dr. Sessler noted. “On the other hand, I was surprised that both wound infection and transfusion requirements were comparable between the two groups. Especially for transfusion requirements, the evidence was quite good over a wide range of time, trials and meta-analyses, all showing substantial effect. But we just saw none in PROTECT.”
In terms of tolerability, 39 adverse events occurred in patients who received aggressive warming (17 serious), compared with 54 among those assigned to routine thermal management (30 serious). One serious adverse event—observed in an aggressively warmed patient—was deemed to be possibly related to thermal management.
“The results of PROTECT are clear: Aggressive intraoperative warming doesn’t reduce the risk of cardiovascular complications, wound infection or transfusions,” Dr. Sessler explained.
“There are lots of guidelines and standards based on 36 degrees,” Dr. Sessler continued. “But it’s important to remember that 36 degrees was pulled out of the air; there is not a shred of evidence to support that threshold. PROTECT clearly shows that’s wrong; the threshold for hypothermia is above 35.5° C. The standards and guidelines need to be rewritten based on 35.5 degrees.
“This is not permission to ignore warming or temperature monitoring, especially since temperature monitoring is also important for malignant hyperthermia, not just for thermal management,” he said. “Most surgical patients still should be warmed, but any temperature above 35.5 is acceptable.”
Important Threshold Identified
Steven M. Frank, MD, was impressed with the findings. “This is a very large, well-designed study done 25 years after the original randomized trials on perioperative patient warming [JAMA 1997;277:1127-1134],” said Dr. Frank, a professor of anesthesiology/critical care medicine, the director of the Johns Hopkins Health System Blood Management Program, and the director of the Center for Bloodless Medicine and Surgery at Johns Hopkins Medicine, in Baltimore.
“I believe the findings that 35.5° C is a threshold below which patients are at increased risk for cardiac events,” Dr. Frank continued. “The original study on this topic, which we did back in 1997, showed increased cardiac events in a cohort of patients that received no warming with a mean core temperature below this threshold [35.4° C], and in PROTECT the mean core temperature was above this threshold [35.6° C].
“In PROTECT,” he added, “they used ‘rescue’ warming to keep core temperature above 35.5° C, but we did not. We have also shown that below 35.5° C in awake postoperative patients and in human volunteers, catecholamine levels are increased up to 500% above baseline, which is the likely mechanism of cold-induced myocardial ischemia [J Appl Physiol 1999;86:L588-L593].”
Dr. Frank reported no relevant financial disclosures. Dr. Sessler reported that PROTECT was partially funded by 3M, although the company withdrew funding halfway through the trial. Dr. Sessler occasionally consults for thermal management companies; those fees are donated to charity.