
A new study from the Outcomes Research Consortium found that preoperative anemia optimization does not seem to reduce the occurrence of major complications after noncardiac surgery.
Nevertheless, the authors noted that they believe more intense, long-term optimization may yet prove to be beneficial in anemic patients.
“There are multiple studies to demonstrate that preoperative and intraoperative anemia are associated with negative postoperative outcomes,” said Alparslan Turan, MD, a professor and the vice chair of the Department of Outcomes Research at Cleveland Clinic. “This is not in question. But I think it’s more important to ask what we can do when we have a patient who is anemic prior to the surgery.
“At our institution, some of our surgeons will occasionally send patients to our blood bank’s preoperative blood management team, which will try to increase their hemoglobin levels so they are optimized for surgery,” he added. As Dr. Turan explained, preoperative hemoglobin optimization also may reduce the need for intraoperative blood transfusion, which itself has been associated with an increased occurrence of major complications.
To help examine the association between preoperative anemia optimization and a composite of all-cause mortality and major complications after noncardiac surgery, the researchers studied the records of all adult patients with documented preoperative anemia who underwent elective noncardiac operations at the institution between 2014 and 2019. Anemia was defined as a hemoglobin concentration less than 12.0 g/dL in women and less than 13.0 g/dL in men in the six months prior to surgery.
The study’s primary exposure variable was preoperative anemia optimization, according to the patient blood management protocol; its primary outcome was a composite of all-cause in-hospital mortality and major in-hospital postoperative cardiovascular, renal and pulmonary complications.
In a virtual presentation during the 2022 annual meeting of the International Anesthesia Research Society, Association of University Anesthesiologists and Society of Critical Care Anesthesiologists (abstract 1096), Dr. Turan reported that the final study cohort comprised 15,104 patients. Of these, 2,295 received preoperative anemia optimization treatment, and 12,809 did not.
Assessment of patients’ median preoperative hemoglobin concentration, which was measured on the closest available date before surgery, was 11.1 g/dL for patients who underwent anemia optimization and 11.8 g/dL for their counterparts who did not undergo optimization. Of note, the mean change in hemoglobin concentration following optimization was 0.0 g/dL for those patients who underwent such treatment; the median length of time between these two measurements was 35 days.
It was also found that preoperative anemia optimization was not associated with the composite outcome. Indeed, the estimated average relative effect odds ratio was 1.02 (95% CI, 0.85-1.23) for anemia optimization versus no optimization (P=0.80). Similar results were found for each component, with no evidence of a treatment-by-component interaction (P=0.17), as the Table illustrates.
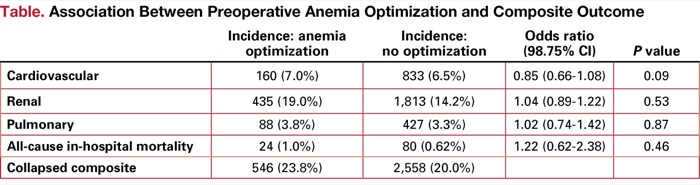
| Table. Association Between Preoperative Anemia Optimization and Composite Outcome | ||||
| Incidence: anemia optimization | Incidence: no optimization | Odds ratio (98.75% CI) | P value | |
|---|---|---|---|---|
| Cardiovascular | 160 (7.0%) | 833 (6.5%) | 0.85 (0.66-1.08) | 0.09 |
| Renal | 435 (19.0%) | 1,813 (14.2%) | 1.04 (0.89-1.22) | 0.53 |
| Pulmonary | 88 (3.8%) | 427 (3.3%) | 1.02 (0.74-1.42) | 0.87 |
| All-cause in-hospital mortality | 24 (1.0%) | 80 (0.62%) | 1.22 (0.62-2.38) | 0.46 |
| Collapsed composite | 546 (23.8%) | 2,558 (20.0%) | ||
“Surprisingly, there was no difference in patients who got optimized in the blood bank and those who did not,” Dr. Turan said in an interview. “Initially, we were thinking that our optimization would work. But clearly, it didn’t.”
However, Dr. Turan said it may be possible to explain why preoperative anemia optimization did not seem to work in this instance. “First of all, it likely depends on when the surgeons are sending the patients for optimization. If they’re sending them only a few days before surgery, that likely will not work well. We need to get these patients in a couple of weeks, or maybe even a month, before their surgeries to see if we can change their hemoglobin levels.”
The results also have left the researchers reexamining their therapeutic approach to preoperative anemia optimization. “The current options we have are not very good and do not give us enough ammunition to solve this problem before surgery,” he said. “Of course, we could give erythropoietin, but it’s very expensive and contraindicated in some patients.”
Nevertheless, that did not stop Dr. Turan from urging his peers to maintain vigilance when faced with anemic surgical patients. “We know anemic patients have worse outcomes; we’ve shown that in a recent paper [Br J Anaesth 2021;126(1):94-101],” he said. Therefore, we believe these patients likely still need to be optimized for surgery.
“However, we still need to figure out what kind of optimization is best,” Dr. Turan continued. “Apparently, the current regimen of iron and vitamins does not seem to address the situation, so I believe anemic patients need to be more aggressively treated to be ready for the surgery and to make a difference in their outcomes.”
Steven M. Frank, MD, a professor of anesthesiology/critical care medicine at the Johns Hopkins University School of Medicine, and the director of the Johns Hopkins Health System Blood Management Program and director of the Center for Bloodless Medicine and Surgery at Johns Hopkins Medicine, in Baltimore, was not surprised by the results of the trial.
“Diagnosing the cause and properly treating preoperative anemia is very challenging,” Dr. Frank said. “I call it the ‘high-hanging fruit’ in a patient blood management program.
“Even when done properly, studies are mixed on whether you can reduce transfusions or improve outcomes,” Dr. Frank continued. “More research needs to be done to define best practices for managing preoperative anemia.