More than 30 years after the National Institutes of Health developed the initial consensus statement on metabolic and bariatric surgery, two of the world’s leading authorities in the field published new, evidence-based guidelines expanding the scope of indications and, potentially, chipping away at the barriers to these powerful surgical interventions.
“We’ve made incredible innovations and strides in all aspects of medicine and surgery, and in metabolic and bariatric surgery [MBS] in particular,” said Shanu N. Kothari, MD, a minimally invasive bariatric surgeon at Prisma Health in Greenville, S.C., an immediate past president of the American Society for Metabolic and Bariatric Surgery (ASMBS), and a co-author of the guidelines (Surg Obes Relat Dis 2022;18[12]:1345-1356).
“Already, we’ve seen on social media anecdotal cases of surgeons who have had denials overturned for patients who meet eligibility according to our new, updated guidelines,” Dr. Kothari noted.
Teresa LaMasters, MD, the medical director of the UnityPoint Clinic Weight Loss Specialists in West Des Moines, Iowa, and current president of the ASMBS, noted that there have been some prior attempts to update the 1991 consensus but that adoption was minimal, especially by insurance companies.
“They hewed to the old guidelines, which I think is residual weight bias and discrimination—kind of unconscious bias. We would never consider using 30-year-old guidelines for cardiovascular disease,” she said.
The new guidelines, a joint project of the ASMBS and International Federation for the Surgery of Obesity and Metabolic Disorders, reflect the safety of MBS and evolution of the understanding of the disease of obesity—a profoundly heterogeneous condition that is better treated sooner rather than later.
“To me, this is the fastest evolving field in all of surgery, and our learning just continues to expand exponentially,” Dr. LaMasters said.
Barham K. Abu Dayyeh, MD, MPH, a gastroenterologist and an internist with expertise in the endoscopic management of obesity and metabolic diseases, said the new guidelines are timely and necessary, especially as the number of people suffering with obesity and obesity-associated diseases continues to grow.
“The criteria set 30 years ago is not sufficient. The prevalence of excess adiposity continues to increase, approaching 50% of the U.S. population being overweight or having obesity. These new guidelines that could increase access to bariatric surgery to a bigger segment of the population are a step in the right direction, and needed in order to get the treatment to patients who need it.”
Shifting Away From BMI as An Indication for Intervention
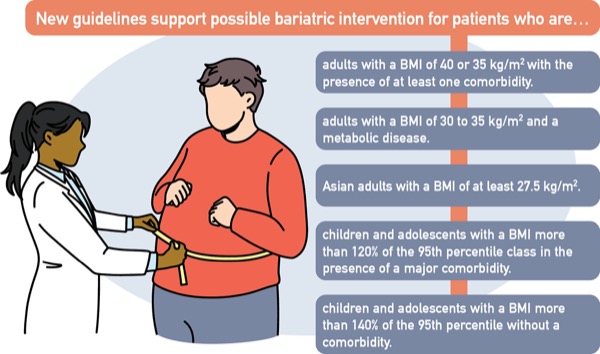
Once limited to patients with a body mass index of at least 40 or 35 kg/m2 with the presence of at least one obesity-related comorbidity, the new guidelines support bariatric intervention for patients with a BMI of 35 kg/m2 with or without comorbidities. It also supports considering MBS in patients with a BMI of 30 to 35 kg/m2 and a metabolic disease such as type 2 diabetes.
“Millions of patients fall into that category, and we know that the earlier you intervene with MBS, the higher the likelihood of long-term remission of the diabetes. We too often see patients after 25 years of type 2 diabetes when they have significant end-organ damage, are at the highest perioperative risk for surgical complications and the lowest chance that the surgery will have a successful impact on their diabetes,” Dr. Kothari said.
The guidelines further suggest that BMI thresholds be adjusted in Asian populations based on the understanding that these patients tend to experience worse disease. The paper establishes a BMI of 25 kg/m2 for clinical obesity and recommends offering MBS to Asian patients with a BMI of 27.5 kg/m2 or higher.
“We know now that diabetes and hypertension are different diseases in the Asian population; they come on at a lower BMI and are more severe. Based on the 1991 NIH guidelines, these populations were being discriminated against by adhering to the previously determined BMI units,” Dr. Kothari said.
Consideration for Patient Selection
Acknowledging that patient selection is critical in older patients, the guidelines state that there is no known upper chronological age limit for MBS; in older patients, the slightly higher risk for surgical complications should be weighed against the benefits of weight loss and remission of obesity-related comorbidities.
At the other end of the spectrum, the guidelines recognize that MBS is safe in patients younger than 18 years of age and has the potential benefit of sparing a patient years or decades of the burden of obesity and its associated comorbidities. They recommend considering MBS in children and adolescents with a BMI more than 120% of the 95th percentile class in the presence of a major comorbidity, or 140% of the 95th percentile without a comorbidity.
Consideration of MBS is also recommended for patients whose future may include joint replacement, organ transplantation or abdominal wall hernia repair; patients whose outcomes would likely be superior if they are able to undergo weight loss first; or who might never make it to surgery without weight loss.
“This is an area where we can help other subspecialty societies in all those respective disciplines. If a patient undergoes MBS and can lose 100 pounds before a hip or knee replacement, we know we lower the operative time for joint arthroplasty and decrease the risk of perioperative complications,” Dr. Kothari said.
The guidelines also indicate MBS should not be withheld from high-risk patients, such as those with BMI greater than 60 kg/m2, and those with cirrhosis or heart failure. As with all the other expanded indications, this recommendation stems, in part, from the well-established safety of MBS.
“I think a lot of people have the misunderstanding that bariatric surgery should be reserved for the worst of the worst, and that’s not true. The BMI guidelines are lower because the safety of surgery has dramatically improved in the last 30 years—a quality success story,” Dr. LaMasters said.
“Part of this is the system of care we have around patients: our preoperative preparation and optimization, plus the multidisciplinary approach to patients both pre- and post-surgery. This is how we do very high-risk patients very safely.”
What’s Next?
It most certainly will not be another 30 years before the guidelines are revised, according to Dr. LaMasters. More likely, revisions may occur within the next five years, which will allow time for an adequate volume of research and literature to evolve.
“I think the new frontier is multimodal therapy, more of an oncology model for the treatment of the chronic disease of obesity. For example, we no longer talk about breast cancer; we talk about an invasive ductal carcinoma, HER2-positive, PR [progesterone receptor]–negative disease. We need that kind of specificity for obesity,” she said.
Although there were no gastroenterologists/endoscopists involved in the creation of these most recent guidelines, Dr. Kothari observed that endoscopic bariatrics is an emerging field, and that there have been collaborative guidelines with GI societies about the role of endoscopy in bariatric patients.
“As the technology advances, the lines will continue to blur between what’s extremely minimally invasive surgery and what’s extremely advanced endoscopy,” Dr. Kothari said.
Dr. Abu Dayyeh said he would welcome future collaboration. “Collective wisdom is important to move the field forward. We need collaboration that involves surgeons, gastroenterologists, endocrinologists, nutritionists and psychologists to address the disease of obesity.
“Bariatric surgery is, in my opinion, a lifesaving intervention. But we have not broken past that 1% to 2% of eligible patients receiving MBS because of the barriers of cost and invasiveness. I think the spectrum of effective therapeutics is going to continue to expand to include anatomy-sparing interventions that work along the same pathway as bariatric surgery and can reach more patients.”
Dr. Abu Dayyeh has received research support from and is a consultant to Apollo Endosurgery, Boston Scientific, Endogenex, Medtronic, Spatz Medical and USGI Medical. Drs. LaMasters and Kothari reported no relevant financial disclosures.