Originally published by our sister publication Anesthesiology News
NEW ORLEANS—A liberal transfusion strategy leads to increased rates of infection in asymptomatic orthopedic trauma patients, according to the results of a prospective randomized study.
The trial found that implementation of a conservative strategy of 5.5 g/dL in such patients led to lower deep infection rates, without any increase in adverse outcomes.
“As physicians, we transfuse a large amount of blood, and it’s definitely lifesaving,” said Leilani Mullis, MD, an assistant professor of clinical anesthesia at the Indiana University School of Medicine, in Indianapolis. “But previous research has also found transfusion to be associated with significant dose-dependent increases in morbidity, mortality and costs. As such, there is ongoing debate what level of anemia should be used as a transfusion trigger for asymptomatic trauma patients no longer in a resuscitative phase immediately following trauma.”
To determine whether a more conservative blood conservation strategy may affect the risk for infection in this patient population, the researchers launched what they call the ORACL (ORthopaedic Trauma and Anemia Conservative Versus Liberal Transfusion) pilot study, which was performed at three Level I trauma centers between 2014 and 2021. The trial comprised 100 adult patients (aged 18-50 years), all of whom required inpatient admission for an associated musculoskeletal injury.

The participants were randomized to either a conservative transfusion strategy of 5.5 g/dL or a liberal strategy of 7.0 g/dL. All of the participants were asymptomatic and no longer being resuscitated at the time of enrollment.
“We had to conduct the study in a non-blinded manner,” Mullis explained. “Because of the low thresholds we were using for the transfusion triggers, we felt that everyone involved in a patient’s care needed to know which arm the patient was enrolled in so they could make sure safety was always a priority.”
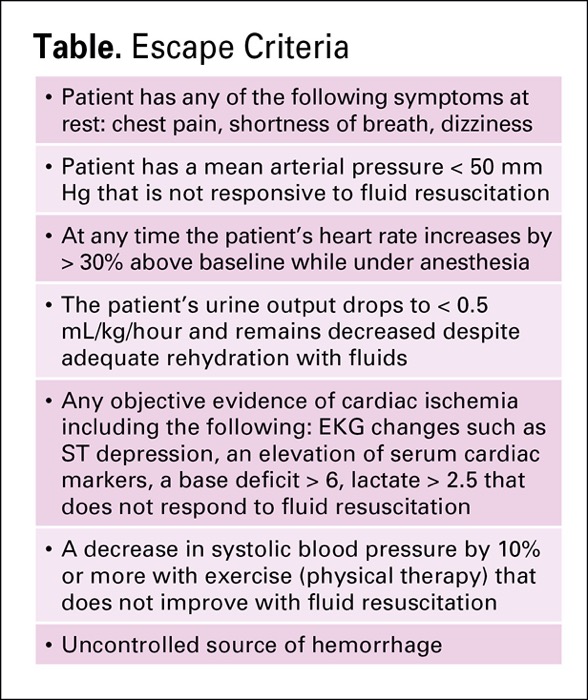
The researchers also incorporated a series of “escape criteria,” which allowed participating clinicians to alter the transfusion management strategy according to a patient’s condition, regardless of randomization (Table).
| Table. Escape Criteria |
|
|
|
|
|
|
|
“That was a very important caveat, particularly for anesthesia,” Mullis explained. “An example would be a patient under anesthesia with a mean arterial pressure less than 50 mm Hg and not responsive to fluid resuscitation, or one with evidence of intraoperative cardiac ischemia with EKG changes or ST depression.”
Liberal Versus Conservative
As Mullis reported at the 2022 annual meeting of the American Society of Anesthesiologists (abstract BOC06), 99 patients completed the 30-day follow-up: 49 in the liberal transfusion group and 50 in the conservative transfusion group. Among these, 14.3% of those in the liberal transfusion group developed an infection within the first month, compared with none in the conservative transfusion group (P=0.0058).
The presence of a deep infection—which the researchers defined as either an unplanned return to the OR for debridement or a hospital admission for IV antibiotics—was also found to be more common in patients undergoing a liberal transfusion strategy (10.2%) than in those undergoing a conservative strategy (0.0%; P=0.0267). By contrast, the incidence of superficial infection, which occurred in 6.1% and 0.0% of patients in the liberal and conservative transfusion groups, respectively, did not achieve statistical significance (P=0.1175).
The two groups proved comparable in terms of multiple secondary outcomes and/or complications that might occur due to anemia or transfusion.
Why Transfusion Increases Morbidity
As the investigators discussed, there are several possible reasons why more patients in the liberal transfusion group experienced infection than their counterparts in the conservative transfusion group.
“Many researchers think the morbidity associated with transfusion is related to the immunosuppression that occurs after transfusion due to downregulation of cellular immunity,” Mullis said. “There are also several studies that have identified the inhibition of natural killer cells and cellular immunity changes with transfusion, though how long these changes persist remains a question.”
The other consideration, Mullis added, is that the current study included trauma patients who were otherwise healthy. As such, the investigators suggested that a more conservative transfusion strategy may prove beneficial in specific patient populations.
“I think in patients who are young and healthy, you can let them run a little more anemic before you pull the transfusion trigger,” she said. “That doesn’t mean that they can have a hemoglobin of 5.5 and be hypotensive and hypovolemic. But I think that you can do it in a safe manner, and maybe lower their infection risk while they’re in the hospital.”
Adequately Powered?
Olubukola O. Nafiu, MD, an associate professor of pediatrics and anesthesiology and the vice chair for academic affairs and research at Nationwide Children’s Hospital, in Columbus, Ohio, raised questions about the transfusion triggers chosen in the study.
“I’m curious to know why you picked that threshold of 5.5 g/dL,” she asked. “I’m also wondering if you looked at body mass index, because we know that obesity is a risk factor for postoperative infection.”
“The 5.5-g/dL threshold was actually not what we initially had hoped for. We had chosen 5.0 g/dL based on previous research,” Mullis replied. “Our institutional review board, however, would not approve the study at 5.0 g/dL, so we compromised and were able to get it approved at 5.5 g/dL. As far as BMI is concerned, that’s not something we’ve looked at, but it’s a good idea to go back and look at that as well.”
By Michael Vlessides
London, Mullis and Nafiu reported no relevant financial disclosures. The abstract was honored as one of the meeting’s best.