
The 8th Annual International Society for Fluorescence Guided Surgery was held on Feb. 20, 2023, at the Biltmore Hotel in Miami. World-renowned experts presented their experience in fluorescence-guided surgery, across a host of surgical specialties. For this and subsequent issues, we present highlights from some of the timely and thought-provoking presentations.
Column Editors
Fluorescence-Guided Surgery: Progressing Toward Safer Pelvic Surgery

CORAL GABLES, Fla.—While the incidence of ureteral injury is relatively low, the most common cause is trauma during surgery, and it can have devastating consequences for patients. Precision while operating in the pelvis is essential, and although there have been attempts to reduce the risk for injury by maximizing visualization, there’s still room for improvement, and agents are in the pipeline that could make a considerable difference, said Sonia Ramamoorthy, MD, at the 2023 annual meeting of the International Society for Fluorescence Guided Surgery.
“There are a lot of agents in trial and they’re exciting. One of these days, we’re going to have a wavelength for everything—the vessels and the ureter and the nerves—because you’ll want to see all those structures to eliminate injury and improve safety in this high-risk area,” noted Dr. Ramamoorthy, a professor of surgery at the University of California, San Diego.
Paradoxically, while minimally invasive surgery (MIS) has revolutionized general surgery procedures overall in terms of morbidity and mortality, hospital length of stay and cost compared with open procedures, it has made it more difficult for surgeons to identify critical structures in the pelvis, Dr. Ramamoorthy said.
“You’re not putting your hands in and doing gentle dissection, you’re working through the gentle or not-so-gentle claws of a laparoscopic instrument or robot. While the technology allows you to home in on what you want to see in detail, you can lose sight of a ureter, which comes all the way from the upper abdomen and kidney to the lowest parts of the pelvis.”
Furthermore, as surgeons have grown more skilled at laparoscopic and robotic procedures, they’ve taken on more complicated cases—“patients whose disease or past surgeries may result in scarring that obscures our ability to identify important structures,” she said.
Consequently, over a 10-year period, the rate of ureteral injuries has increased with the growing adoption of MIS.
“I would say most surgeons are incredibly safe; it’s more about the amount of time it takes to find these structures so we can get the operation started. Before making any big moves like ligating a major vessel and doing a lymphadenectomy, we’ll want to find our ureters so we can keep them in sight and be sure they’re safe and secure,” Dr. Ramamoorthy said.
What are the current options for doing this? There are a few, with varying levels of success and trade-offs.
“We can hope for the best, that we’ll find the ureter. Or we can convert from MIS to open so we can see. Or we can ask urology to place stents intraoperatively before we begin a case; that takes time, planning and money, and there is some risk of injury. Also, in a minimally invasive field, stents might not be as visible as they are in an open procedure, and stents have gotten softer and more pliable. While those qualities make them less likely to cause injury, they also make them harder to see,” Dr. Ramamoorthy said.
As a result, many surgeons are injecting dyes, such as methylene blue or indigo carmine, in laparoscopic and robotic cases. “We can look for them as we would in open surgery, but the dyes offer no advantage when performing the procedure using MIS techniques,” Dr. Ramamoorthy said.
Surgeons still have to differentiate the ureter, the brightness of dyes can be diminished by adiposity, and dyes may fade out before the surgery is complete.
Then there is near-infrared fluorescence with indocyanine green, which has the advantages of being inexpensive, readily available, and effective at visualizing ureters with a good safety profile. But this approach requires stent placement in most case, and, again, may be obscured in patients with obesity or heavy scarring.
“What we really need is something easy to use that could be delivered via IV and quickly lights up the ureters. Let’s make sure this agent will last throughout a five-hour case, be easy to visualize using our current technology and have a strong safety profile,” Dr. Ramamoorthy said.
Although she’s not aware of any agents being FDA-approved yet, many are in trials to determine proper dosing, and it’s just a matter of time. “That would make a big difference in the surgery we do now,” Dr. Ramamoorthy said.
In the past six months, Dr. Ramamoorthy served as a consultant to Arthrex, Intuitive Surgical and Medtronic.
Preventing Nerve Damage During Surgery: Fluorescence Leads the Way

CORAL GABLES, Fla.—Throughout the history of surgery, some degree of nerve damage has been accepted by surgeons and patients as an unfortunate but largely unavoidable outcome. Now fluorescence-guided surgery may drastically improve surgeons’ ability to identify nerves and other vital structures, thus reducing the risk for debilitating iatrogenic injury, said Fernando Dip, MD, at the 2023 annual meeting of the International Society for Fluorescence Guided Surgery.
“It doesn’t matter the quality of the scope or the quality of the TV that you have. It’s something totally different, and that’s why we are convinced this new technology will change the way we conduct surgery,” Dr. Dip told General Surgery News.
Dr. Dip, a head and neck surgeon and surgical oncologist with the University of Buenos Aires and Sanatorio Otamendi Mirolli, in Argentina, likens this technology to a GPS for surgeons. “It tells you where to go or not to go, and it applies to different kinds of surgical procedures,” he said, citing use of fluorescence to detect sentinel lymph nodes and ovarian cancer in gynecology, identify sentinel lymph nodes in breast cancer surgery, and guide anastomoses in colorectal surgeries.
At his institution, which performs a high volume of head and neck surgeries including thyroidectomies, Dr. Dip and his colleagues conducted research on fluorescence imaging to see if it aids in the recognition of parathyroid glands, which can be inadvertently removed at the time of a thyroid resection.
“We wanted to see if it was useful to help visualize the parathyroid glands. We have four parathyroid glands in the neck close to the thyroid glands. Without fluorescence, we identified an average of 2.4 glands. With fluorescence, however, we saw 3.7 glands. The final analysis showed that this was statistically significant and the potential for improvement and better outcomes is obvious,” Dr. Dip said.

In a multicenter trial, Dr. Dip and Raul Rosenthal, MD, and their colleagues demonstrated that by using indocyanine green (ICG) in combination with fluorescence imaging, they could see three times more of the biliary tract anatomy than they could visualize before while using white light alone. “This is the first time we could see critical anatomical structures that we couldn’t see before unless we utilized sophisticated radiologic techniques,” Dr. Dip said.
This study led the two surgeons to investigate the potential use of fluorescence imaging in intraoperative nerve identification and preservation. “We had established that the technology gives us better visualization and safety, but it would be more impactful if it would allow surgeons to identify nerves. Depending on its location and type, nerve injury could be debilitating and have a detrimental effect on patients’ long-term quality of life.”
Improved identification of nerves was a topic they had given a lot of thought. “We tried to avoid using any kind of drug, dye or probe that companies are currently investigating to make nerves shine, mainly because it takes years before drugs and probes are approved by FDA. In addition, these drugs might have potential for side effects, be expensive, and as such not easily available to the general public.” Dr. Dip said.
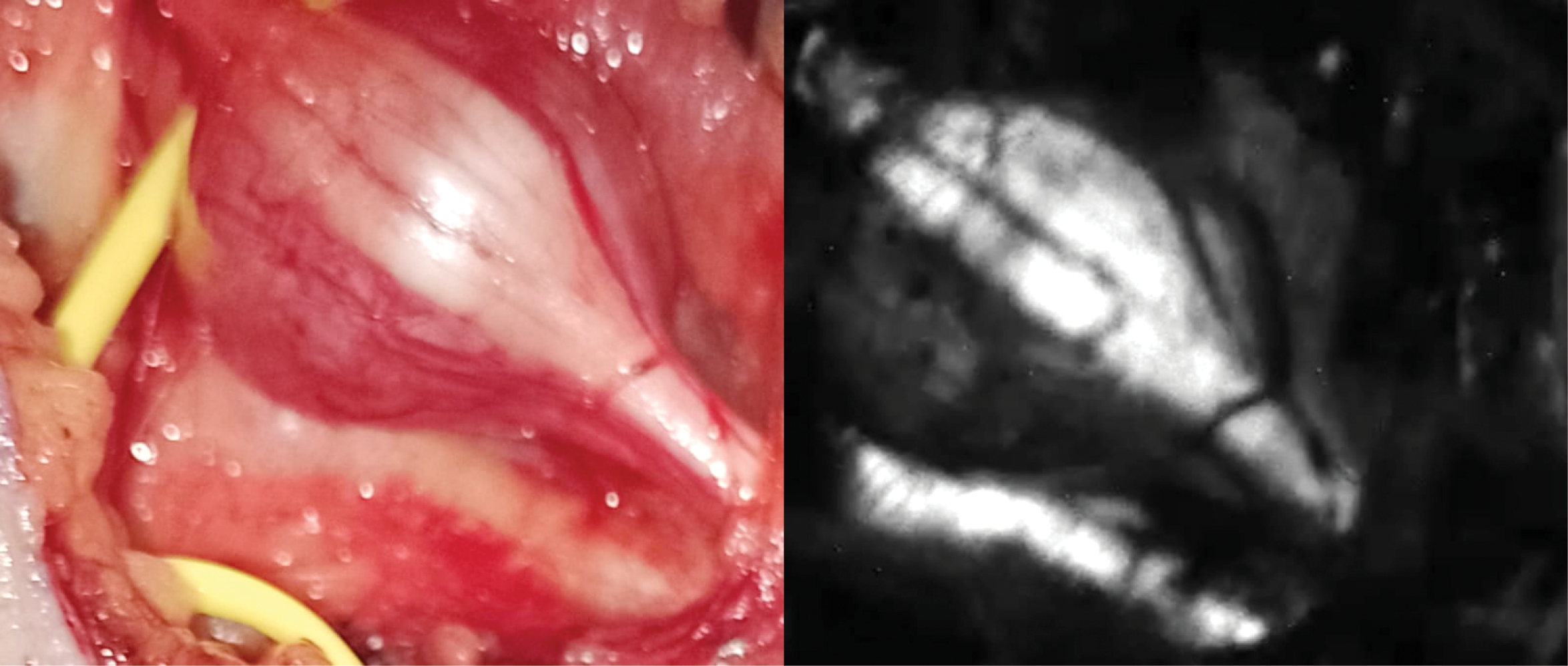
Drs. Dip and Rosenthal started experimenting with ex vivo nerve tissue and different wavelengths, filters and software. “At the beginning of the experiments, working on the bench utilizing a special microscope with a specific wavelength to illuminate nerve tissue, we were able to see the nerves glow—this was really exciting. Then we created a special camera and applied this technology on animals. We were able to visualize nerves but the rest of the tissues we illuminated remained dark. It was then that we realized that we could really differentiate the nerves from other tissues and help prevent or recognize injuries,” Dr. Dip said.
Last year, they published research showing that the intraoperative use of near-ultraviolet light (NUV) was feasible and markedly enhanced nerve visualization in 17 patients undergoing parotid tumor resection, thyroid tumor resection, and surgery for spinal tumors and peripheral nerve damage (Surg Endosc 2022;36:4079-4089). They have now operated on more than 300 patients using this technology.
“I would say that the great advantage of this new technology is that it allows surgeons to see nerves and prevent injuries. It also allows surgeons to recognize nerve injuries and fix those at the time of surgery,” said Dr. Rosenthal, the regional chairman of The Digestive Disease and Surgical Institute at Cleveland Clinic Florida.
Currently, the technology can be used only in open surgery, and it is not yet on the market. But pending FDA approval, Dr. Rosenthal hopes the device—basically a camera with NUV filters—will be market-ready in 2024.
Dr. Dip believes that once patients understand the benefits of fluorescence imaging, they will seek out the institutions and surgeons who use it. “They will ask if you’re going to use fluorescence imaging in their surgery. Just like nobody is going to doubt the laparoscopic cholecystectomy, in a few years, people will assume you’re going to use fluorescent light in order to operate. It’s just a matter of time.”
 The International Society for Fluorescence Guided Surgery (ISFGS) is dedicated to the global advancement of FGS, connecting surgeons, nurses, other allied professionals, and patients, and growing the overall awareness and implementation of FGS worldwide. Visit ISFGS at www.isfgs.org and visit the ISFGS patient portal at imageguidedsurgery.net.
The International Society for Fluorescence Guided Surgery (ISFGS) is dedicated to the global advancement of FGS, connecting surgeons, nurses, other allied professionals, and patients, and growing the overall awareness and implementation of FGS worldwide. Visit ISFGS at www.isfgs.org and visit the ISFGS patient portal at imageguidedsurgery.net.