
Column Editors

Surgical treatment of breast cancer has come a long way since Halsted’s radical mastectomy. The next wave of improvement may be based on advances in imaging that help achieve better safety and cosmetic outcomes, according to Alberto Rancati, MD, the chief of oncoplastic surgery at the University Hospital JosÉ de San MartÍn, in Buenos Aires, Argentina, who discussed the role of fluorescent imaging in oncoplastic surgery at the 2024 meeting of the International Society for Fluorescence Guided Surgery.
“Of course, we need to develop evidence-based algorithms to demonstrate safety and effectiveness, but this is the next step in oncoplastic breast surgery based on imagery decision making,” Dr. Rancati told General Surgery News.
While decisions about reconstruction type and timing were once more based on the surgeons’ experience—what the surgeons were comfortable performing—the basis for these decisions is now the patient’s anatomy and evidence supporting reconstruction for that particular anatomy.

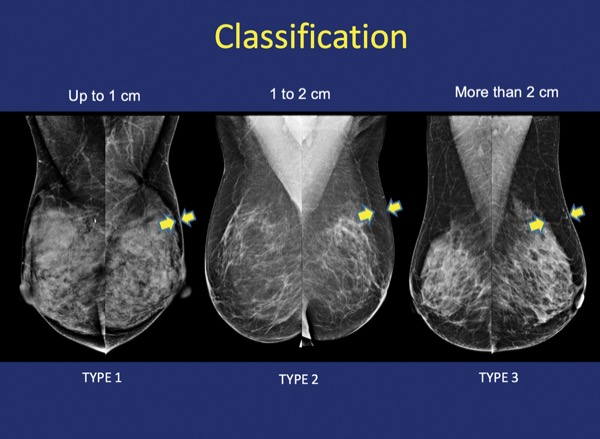
“For example, when the patient’s fat layer between the skin and gland is at least 2 cm, they may be a good candidate for immediate reconstruction in a pre-pectoral position,” Dr. Rancati said.
Immediate reconstruction is the latest standard of care in breast cancer patients, as it allows for treatment of the disease while simultaneously obtaining the best cosmetic result. Identifying patients who are appropriate candidates for immediate reconstruction requires use of multimodal imaging, modalities that include mammography, MRI and now fluorescent imaging, he said.
“When you administer indocyanine green [ICG] intravenously, it binds to plasma protein. The ICG is activated by near-infrared light, which allows you to see angiography in real time.”
This preoperative fluorescence-guided imaging allows for the visualization of vascular flow, identification of vessels surrounding the tumor and of pedicles that will make the best flap for reconstruction, and to plan vascularization of the nipple-areolar complex, he said.
It also helps identify patients who are not strong candidates for immediate reconstruction.
“You can also see where the vascular flow is interrupted by previous biopsy scars, which makes it easier to identify high-risk patients and mitigate possible complications. Some patients are not good candidates for immediate reconstruction in one stage. In these patients, we may be able to do reconstruction with expanders followed by an implant.”
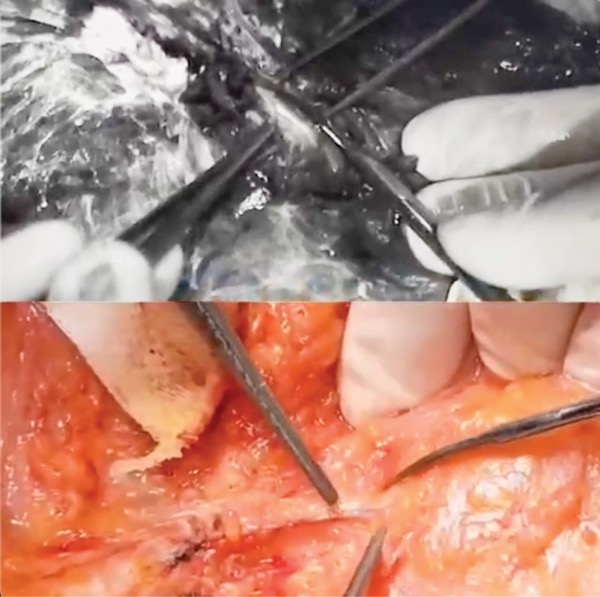
Dr. Rancati and his colleagues are also using fluorescence-guided surgery to preserve sensation in the breast after surgery and reconstruction, using ultraviolet light to detect nerves, which autofluoresce when exposed to that wavelength.
“We use infrared light with ICG and ultraviolet for nerves; the combination of these two allows us to make decisions based on imaging. There are a lot of techniques to repair nerves with grafts taken from different parts of the body, but if you can see the nerves, you can preserve them, which is better than a graft repair,” Dr. Rancati said.
He advised younger surgeons to learn this new technology, and more advanced surgeons to adopt it as part of their ongoing progress as surgeons. “We need to move forward in surgery and not repeat techniques from a century ago. We are changing the surgical arena, and I think in the near future we will have a lot of evidence to compare rates of complication before and after these advances were made,” Dr. Rancati said.