Originally published by our sister publication Gastroenterology & Endoscopy News
PHILADELPHIA—An on-demand telehealth program redirected an overwhelming 90% of gastrointestinal-related emergency department visits, expanding access to care and saving money, during a recent pilot study.
“Digestive disorders represent the leading cause of treat and release from U.S. ERs, resulting in significant healthcare expenditures,” said Naresh Gunaratnam, MD, of MNGI Digestive Health, in Minneapolis, presenting the data at ACG 2024 (presentation 42). Telehealth offers a potential solution, according to Dr. Gunaratnam and his co-investigators. In their short telehealth pilot, conducted from Jan. 24 to April 12, 2024, they estimated savings of more than $400,000.
The study involved established patients at a community single-specialty GI practice with clinics in and around the Seattle/Tacoma area. Integrated telehealth services were provided via the on-demand telehealth platform WovenX Health, which connected patients with advanced practice providers (APPs) supervised by board-certified gastroenterologists. The most common referral sources were the GI practice call center (42%), triage nurses (21%) and the GI practice website (24%), which invited patients seeking immediate attention to schedule an appointment through the platform. The median wait time for an appointment was less than six minutes, and the median visit length was 21 minutes. Patient survey data indicate a high level of satisfaction with the telehealth service, although the survey response rate was only 14%.
Among the 501 patients who participated in the program, 65.9% were women and the average patient age was 53 years. Dr. Gunaratnam said 98% of patients were deemed appropriate for an initial telehealth encounter with a board-certified gastroenterologist. Although 44% of patients reported that they were considering seeking emergency or urgent care before the telehealth visit, only 2% of patients were directed to do so at the conclusion of the visit, Dr. Gunaratnam said. He added that another 35.7% of patients reported that they would have consulted with their primary care providers and 18.2% that they would have sought an appointment with another GI provider.

The most common diagnosis among patients using this service was abdominal pain, at 27.4%. Other diagnoses included gastroesophageal reflux disease or dyspepsia (10%), dysphagia (8.6%), diarrhea (7.9%), inflammatory bowel disease (7.7%), constipation (7.7%), rectal bleeding (4.7%), nausea/vomiting (3.4%), and diverticular disease (2.4%).
Expanding Access to Care
Expanding access to care was an important impetus for the pilot program. “One of the things that is really more of an existential issue for me, what I didn’t see being solved, was the access problem,” lead study author Russ Arjal, MD, said, adding, “we should focus as much on errors of access as we do on diagnostic errors.”
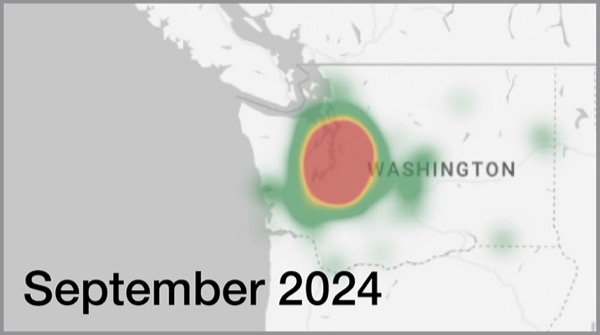
The findings show that telehealth can offer a solution to improve access. Over the course of the study, the researchers were able to use telehealth “to expand the geography” of care, as illustrated by a coverage map showing how patient location expanded south and east into Washington state, Dr. Gunaratnam said (Figure).
“This is a great example of how practices are implementing innovative solutions to address workforce shortages and patient access to specialty care, especially in rural communities,” Kathleen Teixeira, the American Gastroenterological Association’s vice president of public policy and advocacy, told Gastroenterology & Endoscopy News. “APPs can help triage and care for patients and enable gastroenterologists to focus on more complicated patients.”


But Ms. Teixeira stressed that the potential of telehealth to improve and expand care may be limited if Congress does not re-authorize the Telehealth Modernization Act. The AGA has released an issue brief in support of the Act, which must be re-authorized by the end of March for key components enacted during COVID-19—guaranteeing access to and fair reimbursement for telehealth regardless of a patient’s geographic location—to be included. Ms. Teixeira warned that if Congress doesn’t authorize funding for telehealth, “patients will either go without care or seek care in a more expensive emergency department setting.”
‘Speed Matters in GI’
Dr. Arjal, the chief medical officer of WovenX Health, said this study, at least in part, was motivated by a difficult clinical experience. A software engineer in his mid-40s reported rectal bleeding that he suspected were hemorrhoids to his primary care physician, who then referred to Dr. Arjal. The man was concerned and wanted an appointment but was busy, had many competing priorities and became frustrated by wait times. By the time he got a colonoscopy about six months later, he was diagnosed with metastatic rectal cancer, Dr. Arjal said. The husband and father of two was dead within a year.
“It just opened my eyes to how hard it is to get in, even for somebody with resources. Speed matters in GI,” Dr. Arjal said. “It took way too long to see me. I saw a lot of negative outcomes, not from some sort of diagnostic error but, really, just an access error, where people couldn’t get in, and it took three months, four months, and a lot of things can go wrong.”
An Integrated Approach to Rural GI Care
PHILADELPHIA—A three-pronged approach using telehealth, mobile clinics and the integration of gastroenterology into primary care significantly improved access to care while reducing time to diagnosis, hospitalization rates and symptom severity, according to study data presented at ACG 2024.
The project, led by Adebolanle Ayinde, MD, MPH, a second-year resident at Texas A&M School of Medicine, in Longview, was implemented in a rural area in northern Saskatchewan over a 12-month period. The investigators, who won a Presidential Poster Award (abstract P4929), evaluated data from electronic health records, patient surveys and system logs to measure the effect of the three-pronged approach on delays in diagnosis, disease progression, technological challenges, and travel frequency and cost.

Over the course of the year, time from symptom onset to diagnosis decreased by 30%, from an average of 90 days to 63. In addition, Dr. Ayinde and her co-investigators found a 32% decrease in average symptom severity scores as measured on a 10-point scale, from the baseline score of 7.8 to 5.3. Hospitalization rates due to GI complications also decreased 35%.
Dr. Ayinde told Gastroenterology & Endoscopy News that patients in rural settings often must travel long distances for appointments, so transportation can be a significant barrier to care. This integrated care model reduced out-of-community travel by 75%, from an average of four visits per patient per year to one visit per patient per year, saving each patient an average of 200 miles of travel.
The technology required to implement an effective telehealth program can be a challenge in rural environments, Dr. Ayinde said, so it was important to devote resources to ensure that patients had access to high-speed internet and technological support when issues inevitably arose. These efforts paid off, she added, given that 85% of patients and 90% of providers reported positive experiences.
“There are many challenges that people who live in hard-to-reach areas experience when it comes to accessing GI services,” Dr. Ayinde said. “This model was a success, and this was evident in enhanced access to GI care, decrease in symptom severity, decrease in healthcare costs, higher user satisfaction with telehealth services and decrease in in-person travel. We are hoping future studies are able to validate this model’s effectiveness, improving GI delivery on a larger scale.”
—K.P.
What’s Next?
Dr. Arjal emphasized that telehealth completely in the cloud is neither advisable nor the goal of this study. He emphasized that virtual care is not a replacement for brick-and-mortar GI services. “When we started, our thesis was that we had to integrate with a GI group. We couldn’t just be a clinic in the sky.”
Underscoring the importance of personal relationships with healthcare providers, which, she said, patients often prefer, symposium moderator Felice Schnoll-Sussman, MD, the director of the Jay Monahan Center for Gastrointestinal Health at NewYork-Presbyterian/Weill Cornell Medicine, in New York City, asked Dr. Gunaratnam whether patients would have preferred a same-day in-person appointment over a virtual one.
Dr. Gunaratnam said that, unfortunately, same-day appointments rarely are available, and wait times for appointments often extend for months. Integrating telehealth is an efficient way to ensure that the patients who need immediate care are prioritized.
“One of the criticisms that I think is warranted is that telehealth can fragment care. It’s an additive expense and another provider,” Dr. Arjal said. “My hope is that data will show how we should construct these programs. I think it will be hybrid programs that really benefit patients.”
The study has continued, and the investigators have submitted a manuscript that includes a much larger data set of about 2,000 patients and nearly 2,200 patient encounters, which includes established patients as well as people new to the practice. Dr. Arjal said the “diversion effects from the ED are even more pronounced with this larger data set.”
—Katie Prince
Drs. Arjal and Gunaratnam reported no relevant financial disclosures.