


Welcome to the September issue of The Surgeons’ Lounge. In this issue, Omar M. Ghanem, MD, FACS, an associate professor of surgery at Mayo Clinic, in Rochester, Minn., discusses the case of a patient referred for evaluation for metabolic and bariatric surgery and her individualized chances of achieving type 2 diabetes remission. Dr. Ghanem speaks with Wissam Ghusn, MD, a PGY-2 surgical resident in the internal medicine program at Boston Medical Center.
We look forward to our readers’ questions and comments.

Sincerely,
Samuel Szomstein, MD, FACS
Editor, The Surgeons’ Lounge
Szomsts@ccf.org
@YANKEEDOC44

Clinical Scenario
A 52-year-old woman with a five-year history of type 2 diabetes mellitus (T2D), a body mass index of 46 kg/m2, a baseline hemoglobin A1c of 7.8% and a fasting plasma glucose of 138 mg/dL is referred for evaluation for metabolic and bariatric surgery. She is currently managed on insulin alone, without any oral hypoglycemic agents. She has diabetic retinopathy but no macrovascular complications. After multidisciplinary assessment, the options of Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy are discussed. The patient and her providers are interested in understanding her individualized chances of achieving postoperative T2D remission.
Prediction Models
Wissam Ghusn, MD: Given this patient’s clinical profile, how would the Diabetes Remission Index (DRI) help guide her counseling regarding the likelihood of T2D remission after surgery (Figure 1) (https://newsnetwork.mayoclinic.org/dri-calculator)?1
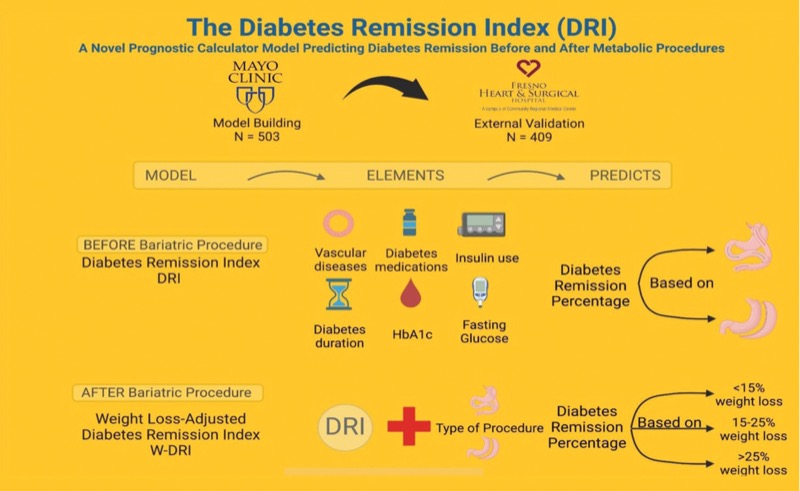

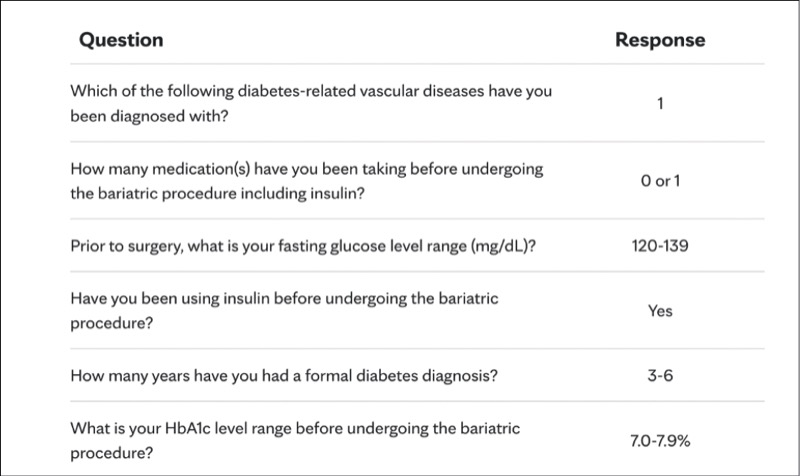
Omar M. Ghanem, MD, FACS: The DRI model incorporates several key preoperative factors: duration of diabetes, insulin use, presence of vascular complications, number of diabetes medications, baseline HbA1c and fasting plasma glucose. In this patient’s case—five years of T2D, insulin use but no oral agents, retinopathy without macrovascular disease, HbA1c of 7.8% and fasting glucose of 138 mg/dL—her DRI score would demonstrate a 31.5% to 39.3% chance of remission after sleeve gastrectomy and a 50.2% to 58.0% chance after RYGB. These figures should guide a shared decision-making process between the provider and the patient. The scoring parameters are seen in Figure 2.
Role of Weight Loss
Dr. Ghusn: In patients like this, with an intermediate preoperative probability of remission, how critical is achieving a more than 25% total body weight loss (TBWL) postoperatively in shifting their predicted remission outcomes per the Weight Loss-Adjusted DRI (W-DRI) model?
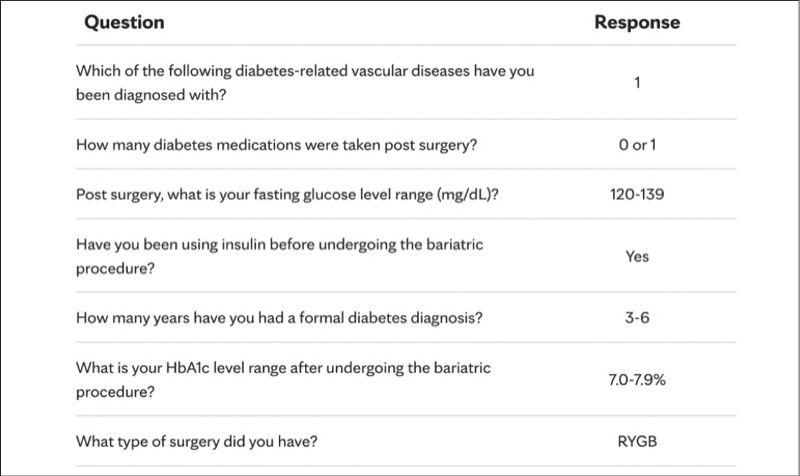
Dr. Ghanem: While her baseline DRI already indicates a moderate to high probability of remission, achieving more than 25% TBWL can still significantly enhance her chances. According to the W-DRI model, patients in this DRI range who achieved greater weight loss saw significant improvements in remission likelihood compared with those who did not. If this patient undergoes RYGB, exceeding the 25% TBWL threshold could raise her post-RYGB remission probability to 59.4% to 67.2% compared with only 23.7% to 31.6%, emphasizing the role of postoperative adherence and long-term lifestyle changes in maximizing benefit. The scoring parameters are seen in Figure 3.
Clinical Practice Implications
Dr. Ghusn: How might tools like the DRI and W-DRI affect your preoperative discussions and shared decision-making with patients considering bariatric surgery?
Dr. Ghanem: Tools such as the DRI and W-DRI help individualize patient counseling by anchoring surgical expectations to objective preoperative and postoperative metrics. For this patient, her relatively short diabetes duration, isolated microvascular disease and modest glycemic elevation contribute to a favorable baseline score, offering reassurance. These tools also support a transparent, data-informed conversation around the differences in remission probability by procedure and the modifiable influence of weight loss, which is critical to patient motivation and engagement.
Future Perspectives
Dr. Ghusn: What future developments do you foresee in enhancing prediction models for diabetes remission, such as incorporating genetic markers or real-time metabolic metrics?
Dr. Ghanem: As the field progresses, models will likely evolve to incorporate continuous physiologic and genomic data. Metrics such as early postoperative glucose trends, insulin resistance markers, C-peptide levels and polygenic risk scores could improve precision in forecasting outcomes. The eventual goal is a dynamic, personalized prediction tool that adjusts in real time based on evolving patient data, allowing for more targeted follow-up and earlier intervention when needed.
Reference
- Ghusn W, Ma P, Vierkant RA, et al. The Diabetes Remission Index (DRI): a novel prognostic calculator model predicting diabetes remission before and after metabolic procedures. Ann Surg. Published online February 4, 2025. doi:10.1097/SLA.0000000000006656
This article is from the September 2025 print issue.
Please log in to post a comment
Why do we keep ignoring SADI? I believe Dr Ghanem does them, correct?
Most surgeons are unnecessarily afraid of this procedure- it MUST be in your toolbox in 2026 - even if you only use it for Sleeve conversions!
Bread and butter bariatric surgeons - please go get trained
Especially if you are a robot skilled young surgeon who is sleeve predominant.