

Originally published by our sister publication Anesthesiology News
NEW ORLEANS—Secondary analysis from the PROPPR (Pragmatic, Randomized, Optimal Platelet and Plasma Ratios) study (JAMA 2015;313[5]:471-482) has concluded that higher doses of opioids may be protective against mortality in severely injured trauma patients.
The researchers added that the findings should not be considered causal at this point, since they were the product of a post hoc analysis and opioid dose was not a randomized therapeutic intervention.
“Although our practice strives to be evidence-based, there is currently a lack of clinical evidence regarding the effect of opioid use in acute trauma patients undergoing anesthesia,” said Evan G. Pivalizza, MBChB, a professor of anesthesiology, critical care and pain medicine at UTHealth Houston McGovern Medical School.
“With that in mind, we analyzed data from the PROPPR study to examine the impact of opioid dose on mortality in severely injured patients,” added Dominique T. Levy, BS, a third-year medical student at UTHealth and the study’s lead author. She and her colleagues hypothesized that anesthetics utilizing higher doses of opioids would be associated with a lower likelihood of death in this population.

For its part, the PROPPR trial examined the ratio of blood components in 680 actively bleeding trauma patients during damage control resuscitation at a dozen Level I trauma centers across North America. Of the 680 participants, 526 (median age, 33 years; 88% male) underwent an emergent procedure requiring anesthesia.
Higher Doses Improved Mortality
The researchers used anesthesia start and end times to calculate opioid dose as morphine milligram equivalents (MME) per hour. They then divided the opioid dose into four quartiles: 0 to 2.54 MME (group 1; n=132), 2.55 to 7.39 MME (group 2; n=132), 7.4 to 14.0 MME (group 3; n=130) and 14.0 to 103.0 MME (group 4; n=132). The primary outcome of the analysis was mortality, which was compared among the four opioid dose quartiles at six hours, 24 hours and 30 days after surgery.
“We saw that patients who received the lowest opioid dose were definitely more severely injured and a little older than the other groups, though we adjusted for all these differences,” Levy explained. Indeed, median Injury Severity Score was 33, 26, 25 and 25 in opioid dose groups 1 to 4, respectively, while median age was 40, 32, 30.5 and 32 years, respectively. The data were adjusted for age, gender, Injury Severity Score, PROPPR treatment arm, race, ethnicity and treatment site.
In a presentation at the 2022 annual meeting of the American Society of Anesthesiologists (abstract A2070), the researchers reported that patients who received higher opioid doses demonstrated significantly improved mortality at all three time points (Table).
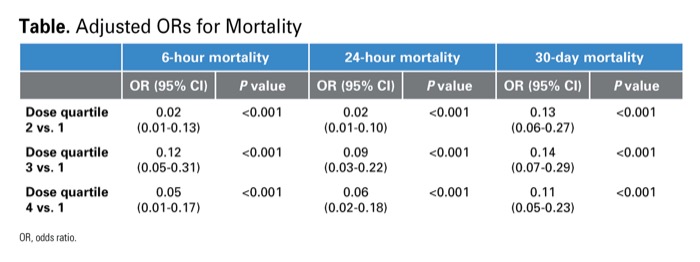
| Table. Adjusted ORs for Mortality | ||||||
| 6-hour mortality | 24-hour mortality | 30-day mortality | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | P value | OR (95% CI) | P value | OR (95% CI) | P value | |
| Dose quartile 2 vs. 1 | 0.02 (0.01-0.13) | <0.001 | 0.02 (0.01-0.10) | <0.001 | 0.13 (0.06-0.27) | <0.001 |
| Dose quartile 3 vs. 1 | 0.12 (0.05-0.31) | <0.001 | 0.09 (0.03-0.22) | <0.001 | 0.14 (0.07-0.29) | <0.001 |
| Dose quartile 4 vs. 1 | 0.05 (0.01-0.17) | <0.001 | 0.06 (0.02-0.18) | <0.001 | 0.11 (0.05-0.23) | <0.001 |
| OR, odds ratio. | ||||||
“We actually took these data and expanded them to look at things like lung and kidney organ injury patterns and systemic inflammatory response,” Levy said. “Interestingly, we had similar outcomes. Patients who received higher opioid doses were protected, although these results were less robust than they were for the mortality outcome.”
However, the researchers were encouraged that their findings shed new light on trauma anesthesia. “I was very impressed with the results,” Pivalizza said. “At this point, we can’t say that giving trauma patients higher opioid doses is going to keep them alive, but we can say that there’s clearly an association. Nevertheless, some trauma anesthesiologists routinely titrate higher doses of opioids to their trauma patients, and I think these findings support that clinical practice.”

Despite the strength of the findings, the investigators recognized that simply administering more opioids to a trauma patient likely plays a very nominal role in 30-day mortality.
“I don’t think we’re [saying] that the opioid exposure is going to be the primary factor driving 30-day outcomes,” Pivalizza explained. “But I still believe the findings support those physicians that may feel uncomfortable at the thought of giving opioids to these individuals. If you want to give high-dose opioids in these acute situations, these results support that decision. We’re all worried about giving opioids, but when appropriate, it seems they can be beneficial in trauma patients.”
Results Not Necessarily Surprising
Albert J. Varon, MD, MHPE, the Miller Professor and Vice Chair for Faculty Development in the Department of Anesthesiology at the University of Miami Miller School of Medicine, was encouraged by the findings. “I find the results of Levy and colleagues’ study interesting, as they ‘vindicate’ my current practice of using high-dose opioids in severely injured trauma patients after volume resuscitation with blood component therapy,” Varon commented. “However, I am not surprised by the results. High-dose opioids were the mainstay of cardiac anesthesia for decades due to their ability to preserve hemodynamic stability and attenuate hormonal and metabolic response to surgical stress.
“The popularity of this technique significantly declined over the years to allow earlier discontinuation of mechanical ventilatory support and fast-track recovery,” he added. “Given the fact that severely injured patients often require postoperative ventilatory support for reasons other than surgery, the use of high-dose opioids in these patients should not be a limiting factor.”
Varon also noted that since the research was a post hoc analysis and not a randomized clinical trial, its results do not prove causation. “Nevertheless,” he added, “their study can be used as the basis for hypothesis generation and future prospective clinical trials.”
By Michael Vlessides
Levy, Pivalizza and Varon reported no relevant financial disclosures. The presentation was selected as one of the meeting’s featured abstracts.
Please log in to post a comment