

Originally published by our sister publication Anesthesiology News

The first study of its kind has found that interindividual variability in responsiveness to propofol anesthesia is associated with inherent differences in brain structure and the function of the frontoparietal networks.
Predicting such responses, the authors said, may ultimately occur before the administration of sedation and general anesthesia, which could help to reduce the incidence of anesthesia awareness. The investigation also identified several novel markers that may also improve awareness monitoring during clinical anesthesia.
“As a neuroscientist, I am very interested in understanding how consciousness changes with anesthesia and why some people become accidentally aware,” said Lorina Naci, PhD, an associate professor of psychology at the Institute of Neuroscience and Global Brain Health Institute at Trinity College Dublin. “Because even though we’ve used anesthesia for over 150 years in clinical medicine to reversibly abolish consciousness, there is a huge individual variability in the way people respond to it.
“What’s more, even if you don’t consider the very rare cases of accidental awareness, up to 25% of individuals have some form of subjective experience, like dreaming or mental cogitation, while they are meant to be completely unconscious,” she continued.

With this in mind, the researchers sought to determine whether three networks integral to conscious cognition—the dorsal attention network (DAN), executive control network (ECN) and default mode network (DMN)—are at the root of responsiveness variability to anesthesia. To do so, they performed two studies [Hum Brain Mapp 2023;44(6):2142-2157].
In the first study, 17 healthy participants (ages 18-40 years; 13 males) were tested in an MRI scanner during wakefulness and during the administration of propofol at dosages of moderate anesthesia. Prior to functional MRI scanning, patient variability in behavioral responsiveness was assessed using an auditory target detection task whereby participants were instructed to press a button with their index finger as soon as they heard an auditory beep through a set of headphones.
Once inside the scanner, participants underwent two functional scans (during wakefulness and moderate anesthesia) while they listened to a five-minute excerpt from the movie “Taken,” wherein a young girl traveling without her family is kidnapped while speaking on the phone with her father.
“We know how the brain responds to narrative,” Naci told Anesthesiology News. “It engages our thinking processes as we try and figure out the plot. So that’s why I used the story; I wanted to see how our thinking—and the brain structures that support thinking—changes as people became less conscious.”
In both cases, three independent assessors measured the participants’ level of sedation using the Ramsay Sedation Scale. For moderate anesthesia, patients received targeted concentrations of propofol as predicted by the Tivatrainer pharmacokinetic simulation program. The infusion commenced with a target effect-site concentration of 0.6 mcg/mL; oxygen was titrated to maintain a blood oxygen level greater than 96%. Throughout sedation, participants remained capable of spontaneous cardiovascular function and ventilation. The mean estimated effect-site propofol concentration during moderate anesthesia (Ramsay 3) was 1.99 mcg/mL, while the mean estimated plasma propofol concentration was 2.02 mcg/mL.
In the second study, an independent group of 25 healthy participants (ages 18-40 years; seven males) were tested behaviorally. In this study, Naci and her colleagues assessed the high-level attention demands of narrative understanding; the results were then compared with the brain activity of participants in the first study who underwent fMRI scanning.
As Naci reported, the first study found significant heterogeneity in response times to the auditory detection task among its 17 participants. Indeed, five individuals were not significantly delayed relative to their wakeful responses, nine were significantly delayed and had fragmented responses, while the remaining three failed to make any responses within the requisite response window (Figure 1).
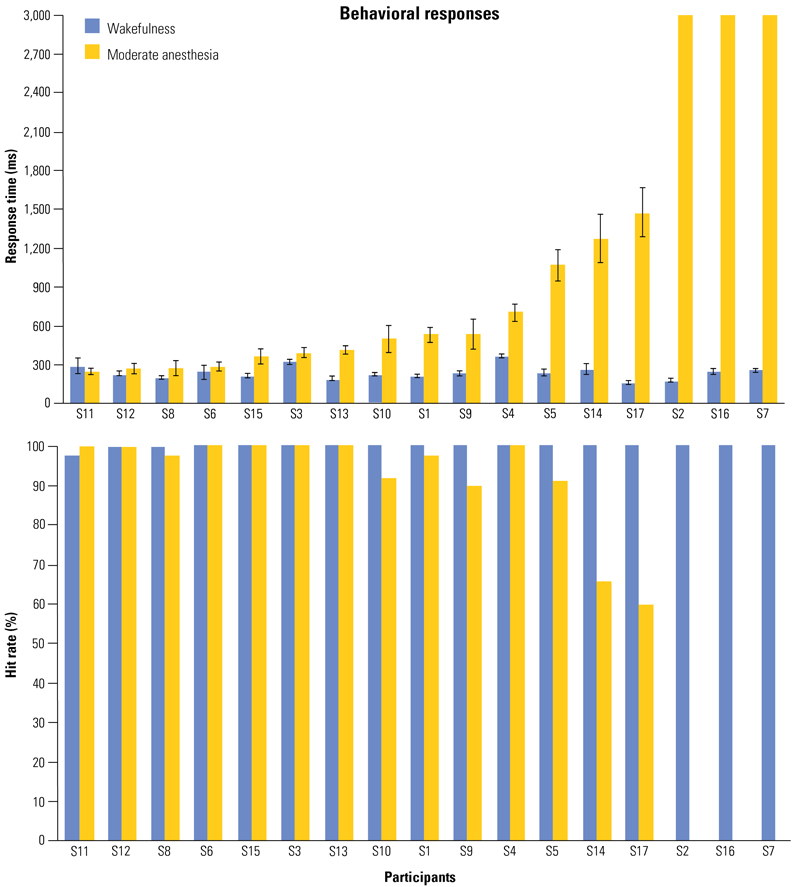
“We found it fascinating that about 30% of the individuals were very fast,” Naci said. “They had received the same amount of anesthetic as the others according to the infusion algorithm, but their response time was not significantly changed from when they were awake.”
Indeed, the large interindividual variability in response times was in direct opposition with the propofol infusion rates titrated for each participant based on the pharmacokinetic model, which adjusted for a host of demographic variables to maintain stable target blood concentrations consistent with a Ramsay 3 sedation level.
These differences, the researchers said, could be explained by one of three possible factors:
- underlying differences in perceptual or high-level attention processes;
- inherent connectivity differences within and between the DAN, ECN and DMN networks; or
- inherent structural brain differences.
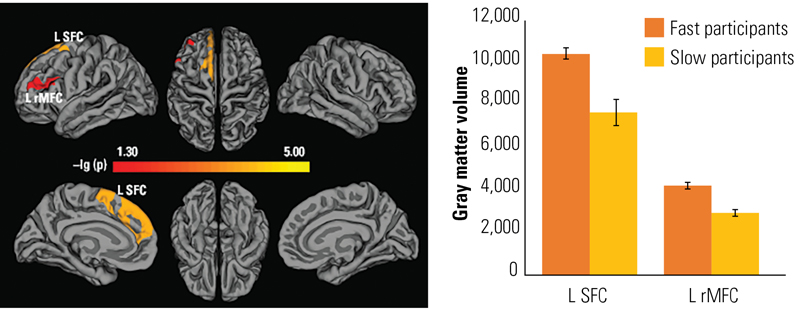
After analyzing the possible effect that each of these factors may have had on the study’s outcomes, the researchers found that interindividual differences could be explained by both structural brain differences and functional connectivity differences. Specifically, fast performers boasted significantly greater gray matter volume relative to slow participants in the left superior frontal region and dorsolateral frontal cortex, as well as the left rostral middle frontal cortex (P<0.0005 for each) (Figure 2). Perhaps not surprisingly, slow participants did not have more gray matter volume than fast participants in any brain region.
Further comparisons in the frontal and parietal aspects of the executive control network showed that functional connectivity within the frontal, but not parietal, aspect of the brain was stronger for fast performers than slow performers during both wakefulness and moderate anesthesia (P<0.05).
“The people whose performance was unchanged were more resistant to anesthesia,” Naci explained. “They not only had structural differences in the parietal cortex, but also demonstrated functional differences in terms of the way the network responded. So the bottom line is there are inherent differences in the people’s brains that predicted how they will respond to anesthesia.”
While the investigators may have anticipated some slight differences between participants’ brain connectivity and their responses while anesthetized, the strength of the correlations—and the structural differences underlying these effects—came as a surprise to them.
“We expected some variability,” Naci said, “but mostly in terms of the extent to which people would be delayed by anesthesia. But what surprised me was that some people just did not seem affected by anesthesia in the way they responded; they were really fast even though they had received propofol and were clinically in a moderate anesthesia state.”
The next, and perhaps most important step in the process, she noted, will be to determine whether clinicians can use these findings to predict individual responses to anesthesia, which may go on to prevent the trauma of awareness.
As Kaman Cipi, MD, the chair of anesthesia at Saint Anthony Hospital, in Chicago, discussed, research efforts such as these may help clinical anesthesiologists further elucidate the brain mechanisms responsible for consciousness.
“The study findings that responsiveness variability during anesthesia is related to differences in brain structure and function of the frontoparietal networks has potential clinical implications,” Cipi said. “The study suggests that individual differences in brain function may affect how patients respond to anesthesia. This knowledge could lead to the developing of personalized anesthesia protocols tailored to individual patients.”
One potential implication, Cipi noted, is the possibility of using preoperative brain imaging to determine patients’ level of responsiveness to anesthesia. “This could improve patient safety by ensuring that each patient receives the appropriate level of anesthesia,” he added. “However, there are some drawbacks to this approach. For example, brain imaging is expensive and time-consuming, and not all patients may be able or willing to undergo this type of testing.”
Another possible implication of the study is the possibility of developing drugs that target the frontoparietal networks to modulate the level of anesthesia. “If such drugs were developed,” he explained, “they could improve the safety and efficacy of anesthesia, as well as reduce the risk of side effects.”
Despite these findings, Cipi noted that more research is needed to fully elucidate the relationship between brain structure and anesthesia response, as well as to develop comprehensive and ethical approaches geared toward using this information in clinical practice.
By Michael Vlessides
Cipi and Naci reported no relevant financial disclosures.
Please log in to post a comment