

—By Caroline Helwick
San Diego—Following a high-quality colonoscopy with negative findings, it may be safe to wait more than 10 years for the next colorectal screening exam, researchers in Poland have found.
Under the right circumstances, the incidence of both colorectal cancer and mortality was reduced out to 17 years, according to the study, which included outcomes observed in more than 200,000 participants in the Polish Colorectal Cancer Screening Program. A negative, high-quality colonoscopy decreased the incidence of CRC by 74% and disease-related mortality by 85%, compared with the general population. In contrast, after a negative but low-quality exam, these reductions dropped to 21% and 60%, respectively, according to the researchers.
“Our results confirm the currently recommended 10-year screening interval, but also suggest that after a high-quality negative examination, the next screening colonoscopy could, perhaps, be safely prolonged beyond 10 years,” said Nastazja Dagny Pilonis, MD, of Maria Sklodowska Curie Memorial Cancer Centre and Institute of Oncology in Warsaw. Dr. Pilonis reported the findings at the 2019 Digestive Disease Week (abstract 571).
More Recent Evidence Lacking
Virtually all specialty societies around the world recommend a screening colonoscopy every 10 years, but these guidelines originated more than 20 years ago and were based on scant data. “The question is, have we gained enough evidence to support the 10-year interval?” Dr. Pilonis asked.

Several studies have hinted at the safety of extending this screening interval; however, they were not conducted exclusively with screening populations and did not account for the quality of the exams, she said.
Dr. Pilonis and her colleagues examined the long-term protective effect of a negative screening colonoscopy after a high- versus low-quality exam. Classification as a high-quality colonoscopy required documentation of adequate bowel preparation, achievement of cecal intubation, and the endoscopist’s adenoma detection rate (ADR) of at least 20%. Researchers also compared outcomes with those of the general Polish population to calculate standardized incidence ratios (SIRs) and mortality ratios.
Of 265,688 men and women screened, 208,428 had a single negative exam and were followed for a median of 10.2 years, and as long as 17.4 years. Rates of CRC and mortality in patients with low-quality exams were twice as high as in those with high-quality exams, according to the researchers (Table 1). They converted the data to SIRs for three time intervals following a negative colonoscopy (Table 2).
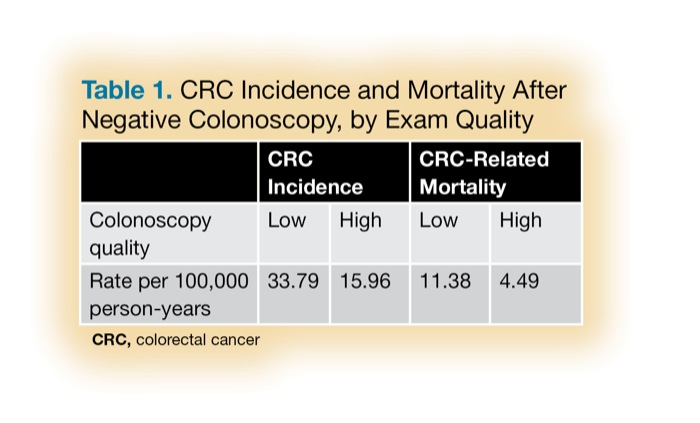
| Table 1. CRC Incidence and Mortality After Negative Colonoscopy, by Exam Quality | ||||
| CRC Incidence | CRC-Related Mortality | |||
|---|---|---|---|---|
| Colonoscopy quality | Low | High | Low | High |
| Rate per 100,000 person-years | 33.79 | 15.96 | 11.38 | 4.49 |
| CRC, colorectal cancer | ||||
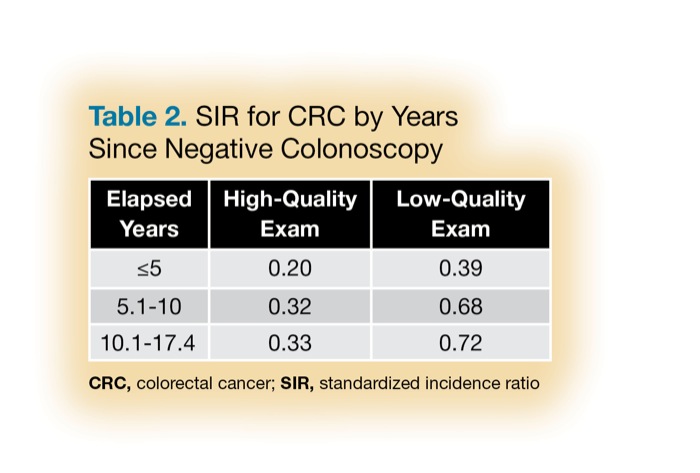
| Table 2. SIR for CRC by Years Since Negative Colonoscopy CRC, colorectal cancer; SIR, standardized incidence ratio | ||
| Elapsed Years | High-Quality Exam | Low-Quality Exam |
|---|---|---|
| ≤5 | 0.20 | 0.39 |
| 5.1-10 | 0.32 | 0.68 |
| 10.1-17.4 | 0.33 | 0.72 |
The critical finding, Dr. Pilonis said, was that the incidence of CRC after a negative, high-quality colonoscopy did not increase significantly during the entire follow-up period. “After a high-quality colonoscopy, the incidence of CRC was not higher between 10 and 17 years, versus the first 10 years after the examination. This is in contrast to a low-quality examination, where there was a significant increase in CRC incidence after the first five years.”
Mortality related to CRC followed the same pattern, with an 85% reduction after a high-quality colonoscopy and a 60% reduction after a low-quality one. Like incidence, CRC mortality did not increase significantly over time in patients having a high-quality negative examination, she said.
For people with any colonoscopy, CRC incidence was significantly lower than that in the general Polish population for the entire follow-up period, she added.
Two experts in CRC screening said the study contributes to a growing body of evidence that examination quality is associated with outcomes. David Lieberman, MD, the chief of gastroenterology at Oregon Health & Science University, in Portland, and the immediate past president of the American Gastroenterological Association, said the key message of the Polish study is “quality makes a difference.”
“The findings emphasize that you need to have a high-quality exam and an adequate ADR. When that happens, and the exam is negative, you’ve identified a very low-risk individual,” Dr. Lieberman said in an interview. “We’ve known from other cohort studies that a 10-year interval seemed reasonable for these persons. The data from the current study extends that to a 16- to 17-year interval. It may lead to a ‘one and done colonoscopy’ for certain individuals.”
Aasma Shaukat, MD, MPH, a professor of medicine at the University of Minnesota and GI section chief of the Minneapolis VA Medical Center, called the Pilonis study “the highlight” of the DDW for her. “It confirms what is being reported by other researchers in a large-scale population-based study: that after a high-quality colonoscopy, screening intervals can be lengthened.”
“Biologically, we know that it takes the adenoma-carcinoma pathway 10 to 20 years to progress,” Dr. Shaukat said. “The main concern for lengthening the screening intervals was quality of the colonoscopy.”
The Pilonis study defines which parameters of high-quality screening colonoscopy confer the same protection up to 15 years, as after 10 years: a complete exam with adequate prep and ADR of 20%. “These quality parameters are not hard to achieve; they are a fairly low bar” that most endoscopists in the United States “meet and exceed,” Dr. Shaukat said, adding she hoped the full manuscript would include differences by patient sex and location of any cancers that develop.
Thomas Imperiale, MD, the Lawrence Lumeng Professor of Gastroenterology and Hepatology at Indiana University School of Medicine, in Indianapolis, agreed. “Other studies have suggested the screening interval could be as long as 15 years. Here, they’ve presented data for a subgroup where physicians had good ADRs and good visualization. It means that for patients with a thorough exam, we think we’ve identified markers of good quality. This study tells us that this works.”
Will the findings lead to a change in screening interval recommendations? “We still need more data,” Dr. Lieberman said. While noting that it will take more than one study to change recommendations, he said the AGA is crafting new guidelines for polyp surveillance that describe the elements of a high-quality colonoscopy. “But this study is compelling,” he said. “Physicians need to pay attention to quality. It really does make a difference.”
Please log in to post a comment